>Corresponding Author : Rajaram Sharma
>Article Type : Case Report
>Volume : 2 | Issue : 3
>Received Date : 30 July, 2022
>Accepted Date : 09 Aug, 2022
>Published Date : 13 Aug, 2022
>DOI : https://doi.org/10.54289/JCRMH2200115
>Citation : Kritika, Sharma R, Tiwari T and Goyal S. (2022) Pediatric Cystic Nephroma with a Review of the Literature. J Case Rep Med Hist 2(3): doi https://doi.org/10.54289/JCRMH2200115
>Copyright : © 2022 Kritika, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access
1Resident Doctor, Pacific Institute of Medical Sciences, Umarda, Udaipur, Rajasthan, India-313001
2Assistant Professor, Pacific Institute of Medical Sciences, Umarda, Udaipur, Rajasthan, India-313001
*Corresponding author: Rajaram Sharma, Assistant Professor, Radio-diagnosis, Pacific Institute of Medical Sciences, Umarda, Udaipur, Rajasthan, India-313001
Abstract
Cystic renal neoplasms have a broader spectrum that includes benign and malignant tumours: benign multilocular cyst, multilocular cystic renal cell cancer and cystic renal cell cancer. Gross similarities in the clinical and radiological imaging findings may cause conflict in their exact diagnosis and further treatment. Cystic nephroma is a rare, non-hereditary benign, multilocular cystic lesion of the kidney and has a prevalence in males. It has bimodal presentation more prevalent in males. In this case patient with cystic nephroma presents with a painless, progressively increasing abdominal lump, which was diagnosed and then operated. Thus, it is crucial to narrow the diagnosis by radiological imaging for preoperative planning and proper management.
Abbreviations: UTI: Urinary Tract Infections, CN: Cystic Nephroma, MLCN: Multilocular Cystic Nephroma, CPDN: Cystic Partially Differentiated Nephroblastoma
Introduction
Cystic nephroma is a very rare, non-hereditary benign cystic renal neoplastic lesion. Various terminologies have been suggested, like multilocular cystic nephroma, multilocular cystic renal tumour, benign multilocular cystic nephroma and polycystic nephroblastoma. Edmunds described it in 1893 for the first time and classified it as cystic adenoma [1]. The bimodal age distribution is observed for cystic nephroma, occurring during the first two years of life and after the 4th decade. During childhood, cystic nephroma constitutes 2-3% of all primary renal tumours [2]. However, it is rare in adults and seen especially after the 4th decade. Adult cystic nephroma shows more incidences in women than men compared to the pediatric age group, which has more males preponderance [2].
The most common presenting symptom is gradually progressive, painless abdominal mass. Multiple urinary tract complaints are observed in symptomatic adults, including abdominal distension, pain, hematuria and recurrent UTI [3].
Asymptomatic cystic nephromas are mostly incidental findings during screening imaging studies. In our case, a four years old female presented with abdominal distention, which was labelled as cystic nephroma on imaging and subsequently confirmed on histopathological examination. A complete radiological workup was helpful in the differentiation of the cystic nephroma with other cystic renal neoplasms.
Case description
A 4-year-old female patient presented with swelling of the abdomen predominantly in the right flank for the last six months. She also had a complaint of diffuse abdominal pain. On clinical examination, a large abdominal lump was palpated in the right flank. No rigidity or guarding was observed. There was no previous history of any abdominal surgery.
The patient was advised for USG abdomen. USG revealed a large cystic lesion with multiple thin echogenic internal septations in the right flank arising from the right kidney (Figure A). The residual right kidney was displaced medially and anteriorly. She underwent a contrast-enhanced CT scan on a 128 slice Siemens machine. On CT, there was a well defined multiloculated cystic lesion of size approx. (12.5 x10.9 x10.5) cm is seen in the right renal fossa. Multiple thick enhancing septations were observed in the lesion. A Claw sign was depicted with the adjacent right kidney suggesting an organ of origin. Residual right renal parenchyma was pushed anteromedially, showing mild hydronephrosis due to pressure effect. Renal vasculature and adjacent great vessels were unremarkable (Figure B, C, D, E). MRI was advised for better evaluation of fat planes with surrounding structures. Multiparametric and multi sequential MRI was performed over a 1.5 Tesla Siemens machine (Somatom 2014 model) using the surface coil. It revealed multiple cysts with thick septations within the lesion. The contents of the cysts appear hypointense on T1 hyperintense onT2WI. No obvious capsular breach/invasion into surrounding tissue was noted (Figure F).
The patient was then operated, and mass was resected (Figure G) and sent for histopathology.
Histopathology reveals multiple variable-sized cystic spaces lined with cuboidal epithelium and hobnail cells (Figure H).
Discussion
CN is a rare benign neoplasm of the kidney with uncertain etiopathogenesis. Edmunds, in 1892, the tumour was initially described as a "cystadenoma" [1]. Since then, multiple theories of the pathogenesis and many terms were given to the CN, including cystic nephroblastoma and benign multilocular cystic nephroma (MLCN). Presently, cystic nephroma is classified as a multilocular cystic renal tumour with cystic partially differentiated nephroblastoma (CPDN). Cystic nephroma and CPDN can be differentiated distinctly by histology but appears identical anatomically and radiologically.
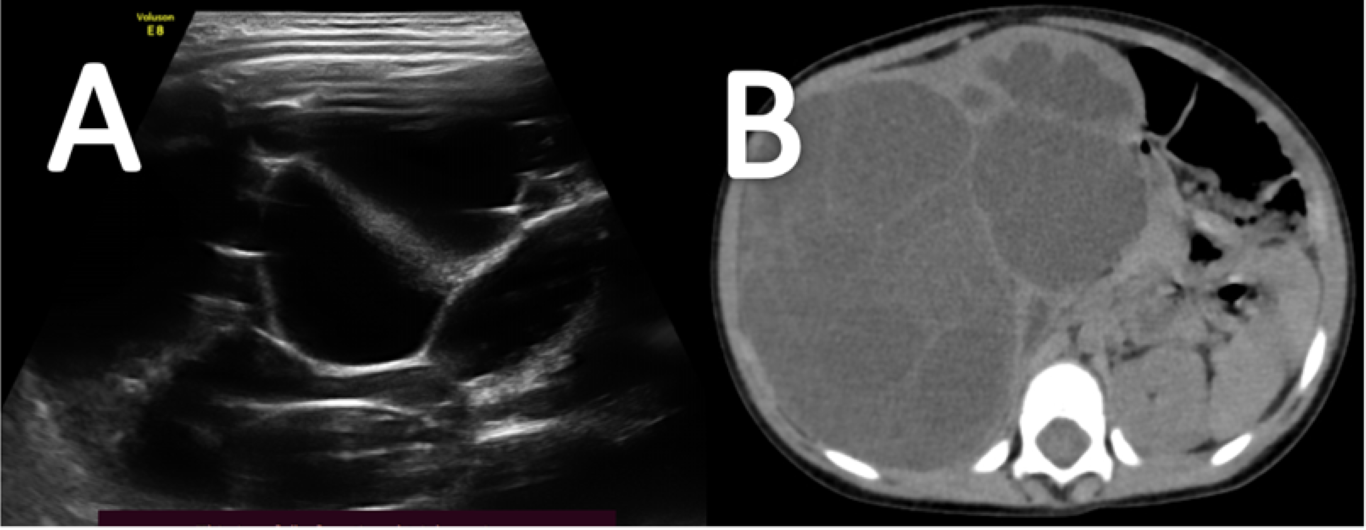
Figure A- USG image illustrates a cystic lesion with multiple internal thick septations.
Figure B- Non-contrast CT axial scan shows a well-defined fluid density lesion showing internal septations in the right renal fossa region.
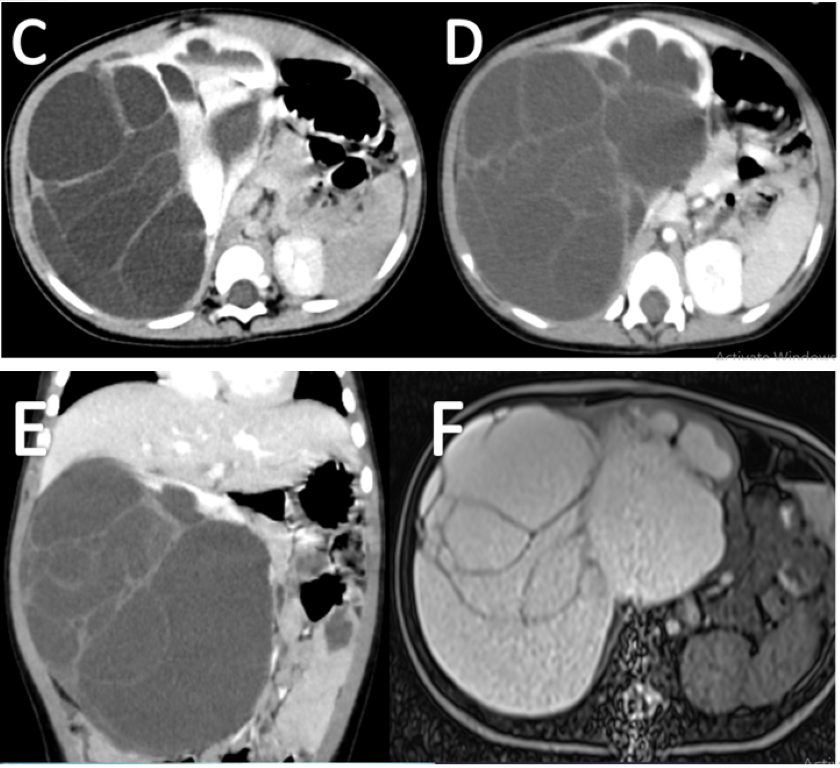
Figure C, D & E- Contrast-enhanced CT scan axial view (C &D) and coronal image (E) shows a well-defined multiloculated cystic lesion with thick internal septations in the right renal fossa region. Residual right renal tissue is seen displaced anteromedially. “Claw sign / Beak sign” is depicted with adjacent right kidney suggesting organ of origin.
Figure F- Non-contrast MRI abdomen T2WI shows a well-defined multiloculated cystic lesion.
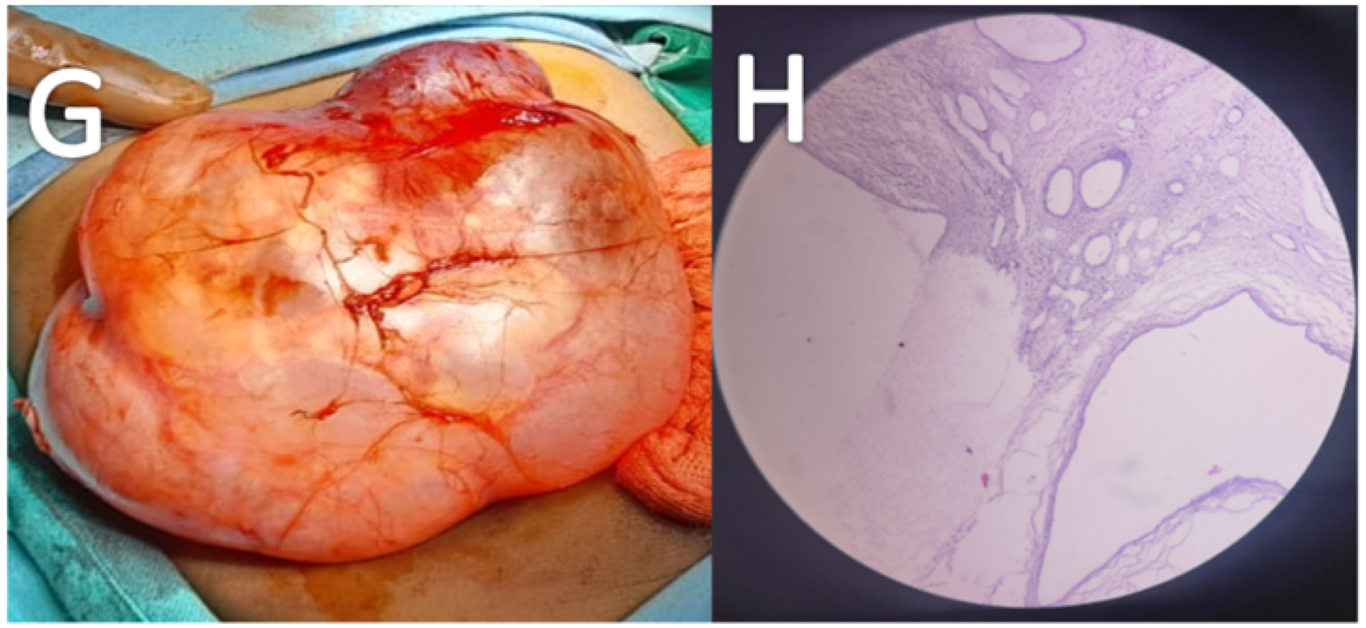
Figure G- Image shows gross specimen post-resection showing large well defined cystic lesion with the multilobulated surface.
Figure H- histology section from kidney illustrates multiple cysts separated by septae. The cysts are lined by cuboidal to hobnail cells. The stroma is composed of fibro collagenous tissue with oedema and mitotic changes.
Gallo and Penchansky [4] reported 2.4% CN cases of 165 primary renal neoplasms at their institution to ascertain CN prevalence. Studies also have observed a biphasic age and sex distribution. Two-thirds of MLCN occur between 3 months to 2 years of age, predominately in the male population, while approximately one-third of cases in the 5th and sixth decades are predominantly in the female population [5,6]. MLCN shows no association with cysts in other organs.
Pediatric patient presents typically with a painless, progressively enlarging abdominal lump in the flank region. The adult population presents with non-specific signs and symptoms such as abdominal pain, hematuria and hypertension. Madewell et al. [6] conducted a review of 58 patients with MLCN at the Armed Forces Institute of Pathology, found hematuria related to urinary tract infection.
Imaging is vital in narrowing the differential diagnosis of the cystic nephroma from other cystic renal masses such as Wilms tumour with cyst formation, clear cell sarcoma, cystic variants of mesoblastic nephroma, and cystic renal cell carcinoma.
The most frequently used imaging modalities in evaluating cystic nephroma are US and CT, which allow preoperative diagnosis, planning, and follow-up. Conventional abdominal radiography (X-ray) shows a significantly large soft-tissue mass with mass effect in the displacement of the bowel. Calcification is usually not seen.
In the US, the renal origin is confirmed by the claw or "beak" signs at the periphery of the mass, displaces the collecting system and shows movement upon respiration. Typically, MLCN appears as multiple cystic spaces separated by thin, echogenic septae. A solid component is usually not seen.
At CT, the locules are typically fluid density. However, it may be seen as slightly hyperattenuating relative to water. Small locules (1 cm) may show myxomatous material within, and the close association of locules with the fibrous septa may cause the mass to appear solid or appear as a solid nodule. The septa enhance moderately (less than in renal cell carcinoma) due to their vascularity [7]. Cystic spaces do not communicate with the pelvicalyceal and collecting system. Cystic lesion displaces the normal residual kidney typically. A variable amount of compression over the collecting system and ureter is possible due to mass effect and may cause hydronephrosis in the normal residual part.
Kettritz et al. [8] studied seven patients and performed MR imaging, confirming the presence of multilocular cystic renal tumours. The presence of fibrotic elements in septae and capsule is confirmed by low signal intensity on T2-weighted MR images [8,9]. Locules demonstrate varying signal intensity due to the presence of protein or blood content. Thin internal septae show typical enhancement after gadolinium administration.
There is a limited role of renal scintigraphy in the diagnosis of MLCN. In the Armed Forces Institute of Pathology series, a total of six patients [4,6] underwent scintigraphy, renal mass appear as a defect. One patient revealed uptake of technetium-99m diethylenetriaminepentaacetic acids by the septa was seen within the mass [4].
Cystic nephroma and CPDN demonstrates gross indistinguishable pathologic features. A well-defined well-encapsulated, circumscribed mass contains multiple non-communicating cystic spaces filled with fluid and distinctly separated by septae. Typically, the mass is unilateral and arises from the lower pole [6], which may occasionally wholly replace the normal kidney. Necrosis and haemorrhage are not seen usually, but herniation of the tumour into the renal pelvis or ureter is usually seen, which may damage the transitional epithelium [6].
Histologically, CNs demonstrate cysts lined with hobnail or squamous, cuboidal epithelium and appear firmly encapsulated (thick, fibrous pseudo capsule). Stromal content shows a close resemblance to ovarian stroma and changes from dense paucicellular collagen to distinct cellular bundles of spindle cells. In Immunohistochemical studies, stromal contents stain mostly with CD10, calretinin, inhibin, estrogen, and progesterone receptors, while epithelial component shows an increased cytokeratin affinity [10].
up to now, there have been no such reports of cystic nephroma demonstrating aggressive local behaviour or of malignant transformation.
Conclusion
Cystic nephroma is a rare entity, accurate diagnosis, which is extremely important for ascertaining its characteristic for preoperative planning and surgical management. CT & MRI depicts meticulous details about its internal characteristic, involvement of renal tissue and surrounding structures that helps in narrowing the differential diagnosis and surgical planning such as nephron-sparing surgery or complete nephrectomy. In cases such as to differentiate MLCN from CPDN, histopathology is helpful.
References
- Edmunds W. (1892) Cystic adenoma of the kidney. Trans Pathol Soc. 43: 89-90. [Ref.]
- Duda-Szymanska J, Kaczmarek J, Papierz W. (2005) Cystic nephroma in adults. A report of two cases and review of the literature. Pol J Pathol. 56: 93-96. [PubMed.]
- Dell’Atti L. (2015) An Unusual Presentation of Cystic Nephroma in an Adult Man. Rare Tumors. 7(2): 5860. [PubMed.]
- Gallo GE, Penchansky L. (1977) Cystic nephroma. Cancer. 39: 1322-1327. [Ref.]
- Banner MP, Pollack HM, Chatten J, Witzleben C. (1981) Multilocular renal cysts: radiologic-pathologic correlation. AJR Am J Roentgenol. 136(2): 239-247. [PubMed.]
- Madewell JE, Goldman SM, Davis CJ, Hartman DS, Feigin DS, et al. (1983) Multilocular cystic nephroma: a radiologic-pathologic correlation of 58 patients. Radiology. 146: 309-321. [PubMed.]
- Dalla-Palma L, Pozzi-Mucelli F, di Donna A, Pozzi-Mucelli R. (1990) Cystic renal tumours: US and CT findings. Urol Radiol. 12: 67-73. [PubMed.]
- Kettritz U, Semelka RC, Siegelman ES, Shoenut JP, Mitchell DG. (1996) Multilocular cystic nephroma: MR imaging appearance with current techniques, including gadolinium enhancement. J Magn Reson Imaging. 6: 145-148. [PubMed.]
- Dikengil A, Benson M, Sanders L, Newhouse JH. (1988) MRI of multilocular cystic nephroma. Urol Radiol. 10: 95-99. [PubMed.]
- Sun BL, Abern M, Garzon S, Setty S. (2015) Cystic nephroma/mixed epithelial-stromal tumour: a benign neoplasm with potential for recurrence. Int J Surg Pathol. 23: 238-42. [PubMed.]