>Corresponding Author : Srikant Agrawal
>Article Type : Case Report
>Volume : 2 | Issue : 7
>Received Date : 10 Nov, 2022
>Accepted Date : 21 Nov, 2022
>Published Date : 08 Dec, 2022
>DOI : https://doi.org/10.54289/JCRMH2200135
>Citation : Agrawal S, Nepal L, Shrestha K, Joshi D, Magar DT, et al. (2022) Missing Hemodialysis Catheter Guidewire and Retrieval Via Inguinal Surgery: A Case Report. J Case Rep Med Hist 2(7): doi https://doi.org/10.54289/JCRMH2200135
>Copyright : © 2022 Agrawal S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access
1Department of Cardiothoracic and Vascular Surgery, National Academy of Medical Sciences, Kathmandu, Nepal
2Department of Critical Care Medicine, Nidan Hospital, Lalitpur, Nepal
*Corresponding author: Srikant Agrawal, Department of Cardiothoracic and Vascular Surgery, National Academy of Medical Sciences, Kathmandu, Nepal
Abstract
Introduction: Hemodialysis catheters are routinely inserted to initiate urgent or temporary hemodialysis. While the procedure is relatively safe, rare complications such as retained guidewire may occur.
Case presentation: We present the case of retained internal jugular vein hemodialysis catheter guidewire in a 25 years old male with acute on chronic kidney disease. The patient underwent one session of unremarkable hemodialysis and remained asymptomatic until the retained guidewire was detected. The intact guidewire was retrieved by the cardiothoracic and vascular surgery team via inguinal surgery on the sixth day of the catheter insertion. No intra- or post-operative complications occurred.
Conclusion: Percutaneous endovascular surgery is preferred retrieval method for retained guidewire. However, in a resource limited setting, open surgical method could be successfully employed to retrieve missing guidewire.
Keywords: Hemodialysis; Retained Guidewire; Surgical Retrieval; Case Report.
Introduction
Hemodialysis is commonly performed therapeutic intervention globally. 82.6% of hemodialysis is initiated with hemodialysis catheter [1] inserted preferably in the right internal jugular vein [2]. The most common immediate complication of hemodialysis catheter insertion is hematoma that occurs in up to 5% of patients while other less frequent but fatal complications are pneumothorax, pneumopericardium, air embolism, guidewire retention, and arrhythmias [3]. Among these, retained guidewire is undoubtedly a preventable iatrogenic complication. Most of the retained guidewire occurs due to inexperience and failure to follow standard protocols. Nevertheless, once identified, attempts to remove retained guidewire must be pursued. We elaborate our experience with a rarely performed alternative method of retrieving missing hemodialysis catheter guidewire via open surgery in a resource-limited tertiary care facility.
Case Presentation
A 25 years old male with hypertension and CKD stage IV presented in the emergency with acute gastroenteritis, acute kidney injury and pulmonary edema due to fluid overload for which urgent hemodialysis with internal jugular vein hemodialysis catheter was planned. Resident Doctor of Internal Medicine performed the catheterization. After completing the catheterization, flow through each port was checked and found normal. One session of hemodialysis was also done which was uneventful. However, when a follow up chest X-ray was done, retained guidewire was identified (Figure 1). Subsequently, an abdominal X-ray was also done (Figure 2). The guidewire extended from hemodialysis catheter lumen to pelvic brim. Intravascular position of missing guidewire was confirmed with USG. An attempt to remove the guidewire by gentle pulling of the hemodialysis catheter failed to retrieve the forgotten guidewire. Therefore, a multi department meeting was conducted. Since endovascular surgery with expertise to retrieve missing guidewire was not available in our centre, consensus was made for surgical retrieval of retained guidewire.
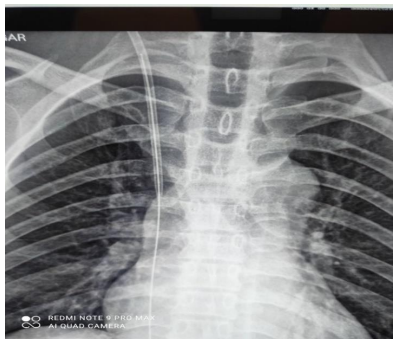
Figure 1: Chest X-ray showing guidewire within hemodialysis catheter.

Figure 2: Pelvic X-ray showing the guidewire extending upto pelvic brim.
In the operating theatre, intravascular position of J-tip of guidewire was confirmed preoperatively with USG doppler and C-arm. Under General Anaesthesia, surgery was performed via inguinal approach. After pre-peritoneal fat layer was reached, extra-peritoneal dissection was continued. Position of J-tip of guidewire was determined with intraoperative USG (Figure 3). Vascular clamps were applied both proximal and distal to the J-tip. Phlebotomy was done in the right common iliac vein. Intact guidewire was retrieved without any complication apart from non-fatal arrhythmia

Figure 3: Intraoperative USG with J-Tip of guidewire in vessel lumen.
Discussion
Guidewire retention is the most common complication occurring with untrained doctors during inadequate supervision [4]. In this case, an inadequately experienced internal medicine resident had performed the catheterization at the end of a busy admission day, albeit with supervision. We infer fatigue and consequent inattention could have resulted in improper handling of the guidewire. Instrument count post-procedure also might have been overlooked. Hence, multiple errors aligned as in a Swiss cheese model for inadvertent retention of guidewire.
When the straight end of retained guidewire is still within the lumen of the catheter, it can be extracted by gentle pulling of the catheter and grasping guidewire [5]. Also, A Cope Mandril, 0.018-inch wire (Cook Medical) can be advanced into the port where the lost guidewire is located, until a tight fit can be achieved and the Mandril can be gently withdrawn to retrieve the guidewire [6]. However, when the end of guidewire is not within catheter lumen, percutaneous endovascular surgery using loop snare is the preferred method to retrieve missed intravascular guidewire [6]. Since such technical expertise were unavailable in our institution, the team of Cardiothoracic and Vascular Surgeons chose an open surgical method of retrieval.
Though multiple case reports of retained guidewire for central venous and femoral hemodialysis catheterization are present, published case reports of retained guidewire during internal jugular vein hemodialysis catheter insertion are limited. Similarly inserted central venous catheter is associated with complications in more than 15% of patients [7] Therefore, we suspect such never events of retained guidewire are under reported. This case report aims to raise awareness of such rare complications to promote procedural safety and suggest possible retrieval methods if such unfortunate events occur.
Conclusion
Hemodialysis catheter insertion is routined procedure, but it needs special attention to details in each step. Retained guidewire is a rare complication and timely retrieval can prevent fatal complications. While minimally invasive endovascular method is preferred method for retrieval, surgical method could be successfully employed in resource limited settings.
Conflicts of Interest: None.
Ethical Approval: Not applicable.
Consent to Participate: Not applicable.
Consent for publication: The patient give us his consent for this publication.
Availability of data and material: The data and material have been used and disseminated legally and transparency.
Code availability (software application or custom code): Not applicable.
Ethical Approval: All the authors approved the manuscript and his contents.
Funding: The authors haven’t receive any financial support for this publication.
Acknowledgement: Consent has been taken from the patient for publication of this case report.
References
- 1. Bream PR. (2016) Update on Insertion and Complications of Central Venous Catheters for Hemodialysis. Semin Intervent Radiol. 33(1): 31-38. [Ref.]
- 2. Lok CE, Huber TS, Lee T, Shenoy S, Yevzlin AS, et al. (2020) KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. American Journal of Kidney Diseases. 75(4 Supplement 2): S1-164. [PubMed.]
- 3. Clark EG, Barsuk JH. (2014) Temporary hemodialysis catheters: recent advances. Kidney International. 86(5): 888-895. [PubMed.]
- 4. Arnous N, Adhya S, Marof B. (2019) A Case of Retained Catheter Guidewire Discovered Two Years After Central Venous Catheterization. Am J Case Rep. 20: 1427-1433. [PubMed.]
- 5. Pralay S, Mubarak K. A lost guidewire - ProQuest. 18(7): 481-482. [Ref.]
- 6. Bream PR, Heffernan DS, Shukrallah B. (2008) Retrieval of a Wire Lost During Central Venous Catheter Replacement. Endovascular Today. 38-41. [Ref.]
- 7. McGee DC, Gould MK. (2003) Preventing Complications of Central Venous Catheterization. New England Journal of Medicine. 348(12): 1123-1133. [Ref.]