>Corresponding Author : Philippe Giaime
>Article Type : Research Article
>Volume : 3 | Issue : 1
>Received Date : 13 Jan, 2023
>Accepted Date : 23 Jan, 2023
>Published Date : 29 Jan, 2023
>DOI : https://doi.org/10.54289/JCRMH2300103
>Citation : Giaime P, Pedinielli N, Chaumoitre J, Mustat A and Sampol J. (2023) Stone Catcher Device to Improve Management of Urolithiasis. Calculstop Trial. J Case Rep Med Hist 3(1): doi https://doi.org/10.54289/JCRMH2300103
>Copyright : © 2023 Giaime P, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Research Article | Open Access
1Clinique Bouchard, ELSAN, Marseille, France
2Phocean Institute of Nephrology, Marseille, France
3Permanences Urgent Care center, Marseille area, France
*Corresponding author: Giaime P, Clinique Bouchard, ELSAN, Marseille, France
Abstract
Urinary stones are a frequent situation, leading to high morbidity and health care costs. As a preventable disease, many diet modifications and sometimes pharmacologic interventions can avoid recurrence. The analysis of the stone is a cornerstone of the diagnosis, but is not made frequently, mainly because of practical considerations for the patients. There is no easy to use device. We tried a new medical device, Calculstop, to catch the stone and keep it safe to the laboratory. We conducted a prospective study in 20 patients, showing 8 times more catching of the stone in recurrent cases. All patients who had catched the stone could have an analysis. The device also facilitated urinary pH measurement. We conclude that the device has been useful to help diagnosis and prevent recurrent stone.
Keywords: Stone Catcher; Urolithiasis; Prevention; Spectrophotometry
Introduction
Urinary stones are a frequent problem. The NHANES study identified that 19% of men and 9% of women will have experienced a urolithiasis at the age of 70 years [1,2]. The main complication is the renal colic, which led to 120 000 admissions in an emergency department in France in 2019 [3], excluding all the cases treated out of the hospital by the general practioner. The prevalence in the whole population increased since the 70’s, from 3,8% between 1976 and 1980, to 5,2% between 1988 and 1994, and 8,8% between 2007 and 2010 [4]. Several risk factors have been identified: age (19,7% of men after 80 years-old, vs 5,1% of men from 20 to 39 years-old), sex (similar incidence before 40 years-old, but more frequent among men after 40 years), race (more frequent in White ascendance), and geography (more frequent in the south-east of the USA) [5]. The studies on the composition of the lithiasis show a high prevalence of calcium oxalate (70 to 80%), calcium phosphate (15%; apatite more frequent than brushite), uric acid (8%), cystine (1-2%), struvite (1%), and others (< 1%) [6]. The recurrence rate is very high, from 10-30% 3 to 5 years after an idiopathic oxalo-calcic lithiasis, and up to 50% at 10 years among men [7,8,9]. The determination of the lithiasis composition is very important because it leads to specific treatment and dietetic advises [8,9] associated with less recurrence [10]. Some urinary biochemical anomalies have been associated with certain types of lithiasis, but the link is sometimes weak. For example, some values as calciuria may have contestable normal range. Phospho-calcic and oxalo-calcic lithiasis share risk factors (low urinary volume, hypercalciuria, hypocitraturia). Hyperoxaluria is a risk factor for oxalo-calcic lithiasis. High urinary pH is a risk factor for phospho-calcic lithiasis, although low urinary pH favors uric acid lithiasis. Moreover, the stone analysis can differentiate the nucleus from the cortical zone, to identify the pathologic process leading to the nucleus formation. For all these reasons, the preventive and curative treatment cannot be based only on urinary biochemical analyses. The morphologic and spectrophotometric analysis of the lithiasis is essential [11]. Several studies insist on the need of these two pillars to make the right diagnosis [12,13,14]. All these data led to a strong recommendation (grade A) of the European Society of Urology to make the morphologic and spectrophotometric analyze, and to measure the urinary pH at the time of the renal colic, even if it is the first episode [15].
Nephrologists often see lithiasis patients after the renal colic. In our experience, we observed a low prevalence of stone analysis, for several reasons: the patient may have not seen the stone, may have not found convenient to catch it with a compress, and sometimes have not been advised of the main interest of this analysis. The measure of the urinary pH at the time of crisis is exceptionally done.
We used a novel device, Calcustop® to facilitate the capture of the stone and its conservation until it is brought safely to the laboratory. It also includes a cycle measurement of the urinary pH. Considering the crisis as a key point in retrieving the kidney stone, we tried to evaluate the interest of Calculstop® as a clinical tool to improve urolithiasis management.
Methods
We conducted a prospective, observational study. It was a feasibility study, not randomized, and not controlled.
It concerned 20 patients treated for symptoms of an acute attack of renal colic in light emergency centers around Marseille, France. If the practioner had a suspicion of renal colic, he proposed the usual treatment (analgesic, and ultrasonography if needed), and gave the Calculstop® kit to the patient with explanations of use.
The kit contained the Calculstop® device to capture the stone, urinary pH sticks with a card to note the results, two bags for conservation, and a notice of utilization.
Emergency situations were excluded (contemporary urinary tract infection, strong pain with inefficient analgesic treatment) because it led to a surgical emergency.
If the patient collected one or more stones, he let them in the device and brought it to the laboratory for infrared spectrophotometric (IP) analysis.
The patients was called by the practionner 7 days later to determine if he caught the stone, sent the stone to laboratory for IS analysis, made the urinary pH measure, and how convenient was the use of the device.
Demographic data were collected.
Ethics: The study design was approved by the French national drug safety agency (ANSM, 23/09/2019), and the protocol by the independent patient’s protection committee (CPP Île-de-France, under n° CPPIDF1-2019-ND63, 13/09/2019). The data processing complies with the health data protection methodology of the French Committee for the protection of personal data (CNIL, n°2213927 v 0, 08/06/2019).
Data analysis: All variables were subjected to a standard descriptive analysis: qualitative data were described in numbers and percentages and quantitative characteristics were described by means, medians, standard deviations (IC=95%). The Chi-2 test was used to compare qualitative variables (gender, treatments, medical history) and the Standard Student's t-test for quantitative variables (BMI, age)
Results
Demographics datas are presented in Table 1.
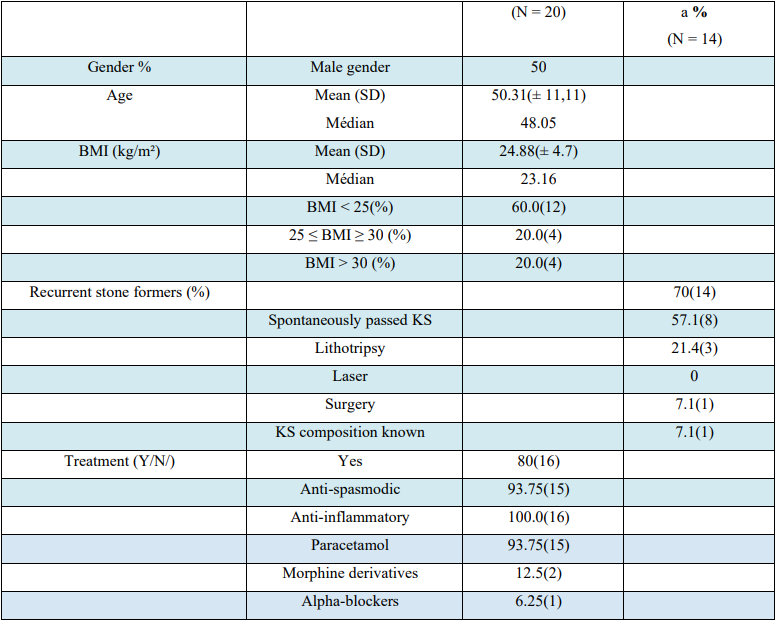
Table 1: Socio-demographic and clinical patient characteristics
a: recurrent stone formers
BMI: Body Mass Index
KS: Kidney Stones
Twenty patients were enrolled during the renal colic crisis, 10 men and 10 women. The BMI was < 25 in 16%, 2530 in 17%, and > 30 in 67%. Seventy percent of patients have already experienced a renal colic. Among them, the lithiasis expulsion were spontaneous (57%), by lithotripsy (22%), by surgery (7%), and no expulsion (14%).
Only 8% of the recurrent patients who expelled the stone (n = 12) had analyzed it previously.
Eighteen patients have been included (2 patients were excluded because they did not answer to the phone call 7 days later). Among the 18 patients, 44% expelled a stone and caught it, 50% did not expelled a stone, and 6% expelled it without retrieving it (Table 2).
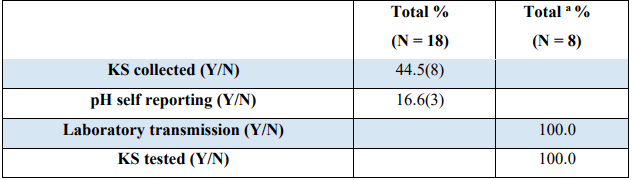
Table 2: follow up
a: KS collected: (N = 8)
Hundred percent of the capture stones (n = 8) were brought to the laboratory and analyzed.
The urinary pH analysis with the stick in the dedicated part of the device was made in 11% of cases.
The kit was judged (Table 3):
• Easy to open and close (100%)
• Easy to use (83%)
• The Laboratory bag was easy to use (100%)
• Instructions were clear for 89%
• 94% considered that the device met their expectations and though satisfied.
• 94% would use it again in case of recurrence.
• 100% would recommend the device in case of crisis to their relatives.
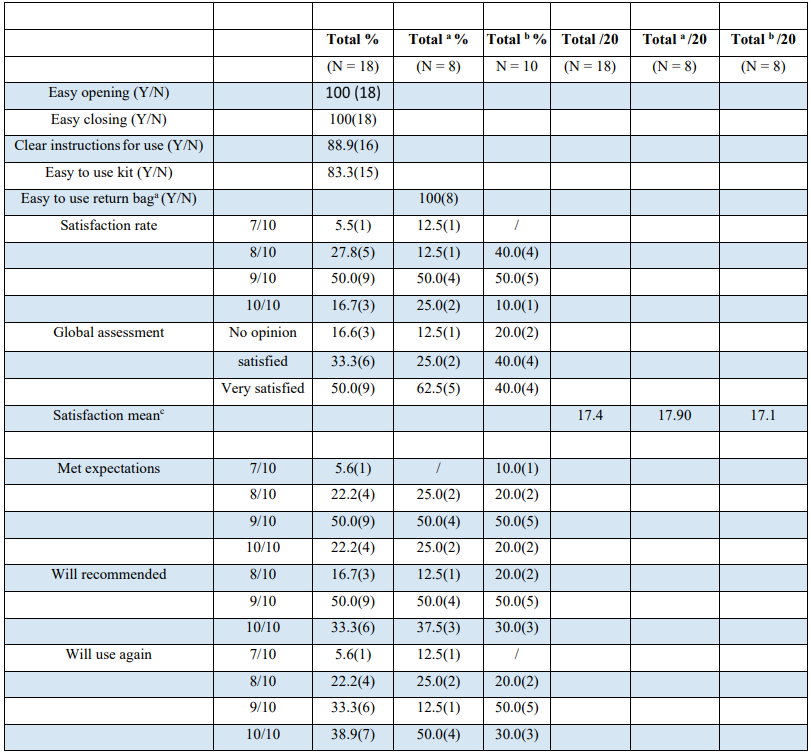
Table 3: Satisfaction surveya
a: KS collected : (N = 8)
b: KS not collected.
c: Mean = {satisfaction rate} + {global assessment}
Discussion
This is the first study addressing the problem of collecting kidney stones. The growing prevalence of the disease, and the heavy medico-economic cost (estimated to 169 million euros in France in 2009) urge the need to improve prevention. Calculstop® device enables 8 times more urolithiasis collection, and 100% analysis of the collected stones. This can significantly improve diagnosis and treatment (diet and medication) of recurrent kidney stones.
Some study shows up to 80% reduction of recurrence with an appropriate treatment.
This observational study was carried out in Marseille, which can be representative of the french standard of living and of the prevalence of renal colic crisis. There is an equal prevalence between men and women, which is a tendency, even if the prevalence in men remains higher in the last studies. There is also a high proportion of patients with IMC>25, which is a known risk factor for urolithiasis.
Among the recurring patients, the majority (57%) had a spontaneous expulsion, which favors the use of a home device. Moreover, only 8% of the lithiasis have been analyzed before, addressing questions about the feasibility of the collection with compress, the understanding of the importance of the analysis, and how to manage the lithiasis once caught.
The study patients were approached through light emergency centers, not equipped with ultrasonography or scanner. Some of the diagnosis may have been biased and may explain the high prevalence (50%) of not-expelled stones.
The urinary pH is of high importance because it partly reveals the biochemical conditions partly due to dietary habits. Once the patient had the crisis, he adapts his diet, and this may modify the results of the biochemical analyses prescribed thereafter. We can note that only 11% of the patients correctly used the pH bandelet, meaning that education about this parameter and modifying in an easier use are warranted.
We found a real satisfaction for the patient using the device. From the understanding to the management of the transportation, patients were satisfied. Most of the evaluated criteria were successfully completed (94 to 100%).
None of our patients reported any adverse effects or events when using the device.
Even with a limited sample of patients and without a control group, there is an overall satisfaction with this collection system, which is integrated with an improvement in patient care. These results need to be confirmed by a prospective randomized control study.
Conclusion
Since renal colic is a growing concern in our societies, the use of a specific device to catch the stone and analyse it may strongly improve prevention by leading to specific diet and treatments options. The goal is to avoid recurrence. The Calcustop® device showed a strong improvement in collection of kidney stones and led to analysis in all these cases.
Bibliography
- Centers for Disease Control and Prevention (CDC). (2021) National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. (NHANES): U.S. Department of Health and Human Services. [Ref.]
- Scales CD Jr, Smith AC, Hanley JM, Saigal CS. (2012) Prevalence of kidney stones in the United States. Urologic Diseases in America Project. Eur Urol. 62(1): 160-165. [PubMed.]
- Letavernier E, Daudon M. (2017) Urolithiasis. Practitioner Review Items. 67(9): e423-e431. [Ref.]
- Stamatelou KK, Francis ME, Jones CA, Nyberg LM, Curhan GC. (2003) Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney Int. 63(5): 1817-1823. [Ref.]
- Chewcharat A, Curhan G. (2021) Trends in the prevalence of kidney stones in the United States from 2007 to 2016. Urolithiasis. 49(1): 27-39. [PubMed.]
- Lieske JC, Rule AD, Krambeck AE, Williams JC, Bergstralh EJ, et al. (2014) Stone composition as a function of age and sex. Clin J Am Soc Nephrol. 9(12): 2141-2146. [PubMed.]
- Hiatt RA, Ettinger B, Caan B, Quesenberry CP, Duncan D, et al. (1996) Randomized controlled trial of a low animal protein, high fiber diet in the prevention of recurrent calcium oxalate kidney stones. Am J Epidemiol 144(1): 25-33. [PubMed.]
- Kocvara R, Plasgura P, Petrík A, Louzenský G, Bartonícková K, et al. (1999) A prospective study of nonmedical prophylaxis after a first kidney stone. BJU Int. 84(4): 393-398. [PubMed.]
- Borghi L, Schianchi T, Meschi T, Guerra A, Allegri F, et al. (2002) Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. N Engl J Med. 346(2): 77-84. [PubMed.]
- Ferraro PM, Curhan GC, D'Addessi A, Gambaro G. (2017) Risk of recurrence of idiopathic calcium kidney stones: analysis of data from the literature. J Nephrol. 30(2): 227-233. [PubMed.]
- Gault MH, Chafe LL, Morgan JM, Parfrey PS, Harnett JD, et al. (1991) Colpitts A Comparison of patients with idiopathic calcium phosphate and calcium oxalate stones. Medicine (Baltimore). 70(6): 345-359. [PubMed.]
- Kourambas J, Aslan P, Teh CL, Mathias BJ, Preminger GM. (2001) Role of stone analysis in metabolic evaluation and medical treatment of nephrolithiasis. J Endourol. 15(2): 181-186. [PubMed.]
- Pak CY, Poindexter JR, Adams-Huet B, Pearle MS. (2003) Predictive value of kidney stone composition in the detection of metabolic abnormalities. Am J Med. 115(1): 26-32. [PubMed.]
- Teichman JM. (2004) Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 350(7): 684-693. [PubMed.]
- EAU Pocket Guidelines. (2021) Edn. presented at the EAU Annual Congress Milan. [Ref.]