>Corresponding Author : Kurt Widhalm
>Article Type : Short Report
>Volume : 3 | Issue : 4
>Received Date : 24 April, 2023
>Accepted Date : 06 May, 2023
>Published Date : 22 May, 2023
>DOI : https://doi.org/10.54289/JCRMH2300119
>Citation : Widhalm K and Stefanutti C. (2023) History of Familial Hypercholesterolemia. J Case Rep Med Hist 3(4): doi https://doi.org/10.54289/JCRMH2300119
>Copyright : © 2023 Widhalm K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Short Report | Open Access
Medical University Vienna, Austria
*Corresponding author: Kurt Widhalm, Medical University Vienna, Austria
Short Report
Familial hypercholesterolemia (FH) is one of the best characterized inborn error of metabolism with an estimated prevalence of 1:250 in the general population. Only approximately 10 % of the affected subjects are diagnosed and therefore under medical care including drug therapy or in severe cases apheresis. Toda data and evidence–based guidelines for detection and treatment are available [1].
Furthermore, in order to prevent atherosclerosis at an early age scientifically based recommendations for preventative strategies have been published [2].
As the first description of FH has been done more than 130 years ago, it is surprising that the knowledge of that very important metabolic disorder is so insufficient. The present report describes historical publications which refer to the clinical and pathophysiological characteristic s of familial hypercholesterolemia.
Background - The discovery of ‚Atherosclerosis‘
A description of arteries likely to be affected by atherosclerosis or arteriosclerosis can be found in Leonardo Da Vinci's drawings and writings, when in 1508, in the Spedale (hospital) of Santa Maria Nova in Florence, performed the famous dissection of the body of a centenary, and drew the old man's arteries comparing them with those of a young man [3].
However, atherosclerosis as nosological entity begun to be named properly after the introduction of the term Ateroma, when the great physiologist Bernese Albrecht von Haller (1708- 1777) published his work, Opuscula Pathologica (1755) [4].
The first two important pathogenic theories date back to the mid 800: the theory of the ‚Crustation‘ of Rokitansky (1842), and the theory of the ‚insudation‘ or ‚inflammation‘ of Virchow (1856).
According to Carl von Rokitansky, atherosclerosis development is due to the formation of small clots stored in the arterial wall, where they undergo to evolution in fibrous tissue. On the other hand, Rudolf Virchow emphasised the anatomical differences between the superficial lipid-related lesions (currently defined „fatty streaks“) and the deeper atheromatous lesions (plaques) [5]. Virchow considered two distinct processes, being the first a case of a simple fatty degeneration, and the second a process in which the fat metamorphosis was preceded by a phase of inflammatory nature [6].
The first descriptions of xanthoma and the association with atherosclerosis
Xanthomas are the main visible clinical signs of familial hypercholesterolemia (FH). The first description of a “xanthoma cardii” was published by G. Lehzen and K. Knauss in 1889 from the Medical Clinic in Würzburg/Germany [7]; they described a 11 yrs old girl, who had yellow spots and lumps on various parts of the body and
who therefore contacted the hospital for help. The family history showed that the parents of the girl were obviously healthy, she had 2 healthy sisters, and one brother. The mother observed also in her younger sister at the age of 9 yrs similar lumps on the body (Fig. 1).
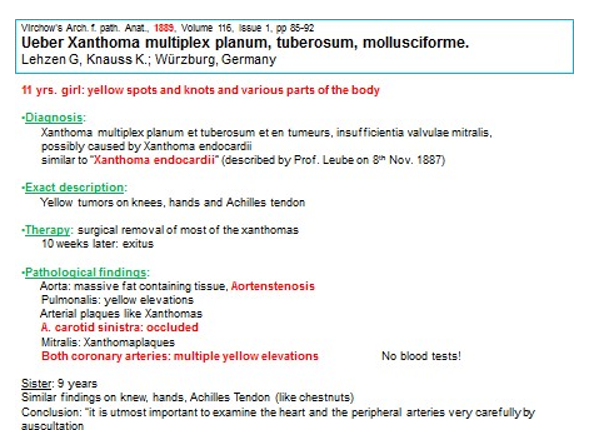
Figure 1
The patient developed at the age of 3 yrs multiple ulcers all over her body; at the age of 4 yrs yellow spots occurred on her eye lids, and one year later prominent yellow lumps on the knees which have since enlarged. Concomitantly similar prominent enlargements occurred on the hands, knees, on the gluteal region and on the feet. On admission to the hospital on 8th Nov 1887 multiple yellow lumps were observed, the consistency was soft, partly “fibromatous”, not connected with the underlying tissue.
On the hands egg- like tumors with yellow- white, partly red color (6 cm - 2,5 cm); furthermore big tumours on the Achilles tendons have been observed.
The examination of the heart showed a soft murmur at the right edge of the sternum; above the heart a long blowing systolic murmur was present, the second pulmonary sound was increased; the diagnosis was : Xanthoma multiplex planum et tuberosum et tumeurs; insufficientia valvula mitralis, possibly caused by xanthoma endocardii .
After a few weeks the tumours in the gluteal region were removed, later on the tumours on the Achilles tendons and on the knees; concomitantly the tumours on hands were removed. 3 1/2 months later the girl collapsed, developed tachycardia and died. The autopsy showed on the aorta a mass of fat- containing tissue, and at the origin of the pulmonary artery yellow prominent spots, similar to the xanthomas.
Above the aortic valves changes of the intima were observed, which resulted in stenosis; the surface of the aorta showed rough protuberances , some similar to sclerotic plaques , some similar to the xanthomas. The left carotid artery was nearly completely occluded, with similar changes to the aorta.
On the mitral valve similar yellow xanthomatous-plaques were present. Both coronary arteries, especially the left, showed multiple plaques; The authors also described the 9 yrs old sister:
She also showed the same lumps and deposits which were typically symmetric; the lumps on the Achilles tendons were the sizeof a chestnut, on her hands the size of peanuts.
The discussion of the nature of this very impressive disease concluded that it should be obligatory in patients with xanthomas to examine the heart very carefully and also the peripheral arteries; they should be intensively auscultated:
This report is probably the first documented description of 2 sisters with homozygous familial hypercholesterolemia: the main clinical signs were xanthomas on the eyelids, knees, elbows and Achilles tendons. What is really amazing is the fact that the authors were able to describe cardiac involvement just with auscultation; the results of the autopsy clearly showed severe atherosclerosis not only in the heart, but also in the carotid artery and the coronary arteries. On this basis the authors recommended that the peripheral arteries should be examined very carefully in all patients with xanthomas.
More descriptions of xanthomatous tumours were published by Tournoux [8] (93 cases Fig.2) and Harbitz (11 cases) in 1927; in the last paper chemical analysis of the tissues revealed fat and presumably cholesterol- esters [9].
Figure 2
The first report that xanthomas were associated with hypercholesterolemia was published by Hoessli in 1914 who found in a 27 yrs old woman with xanthomas on the elbows and on the tendons a blood cholesterol of 528 mg/dl [10].
In a detailed review “de la nature des xanthomes” Louis Török [11] from Budapest summarized more than 40 published descriptions of xanthomas beginning from 1871 with Virchow and ending with Besnier in 1891. Only in few patients has atheromatous involvement been described.
In 1939 the Norwegian physician Carl Müller presented at the Nordic Congress for Internal Medicine in Helsinki for the first time the true entity of Familial hypercholesterolemia as he described 17 families with all the features of xanthomas and coronary heart disease at an early age. In this first description, xanthoma tuberosum, tendon xanthomas and xanthoma palpebrarum were all classified. It is surprising that although the description of clinical signs and the pathological abnormalities were clearly observed and described more than 100 years ago, the majority of affected subjects are not adequately recognized and diagnosed nowadays, although sophisticated methods for clinical diagnosis are available. Müller’s investigations were published in a Supplement of Acta Medica Scandinavica and in the Archives of Internal Medicine 1939 [12].
He was the first to recognize that FH is an inborn error of metabolism with a strong pattern of inheritance.
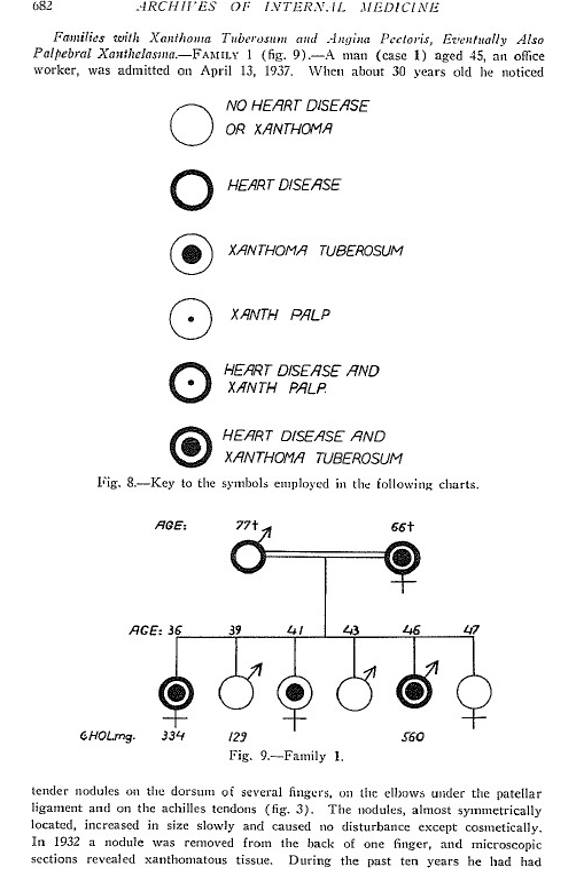
Figure 3: Müller C. Angina Pectoris in Hereditary Xanthomatosis. Archives of Internal Medicine, Volume 64, pp. 675-700, 1939
It is noteworthy that since the first description of FH 130 years ago were gone. Furthermore, it is remarkable that despite great success in research (description of the LDL-receptor, genes and other mechanisms, like PCSK-9 pathway, effective drugs and apheresis) most of the affected patients are not detected today. This fact should stimulate us to increase all efforts to improve the knowledge about FH in all physicians, but also in potential patients.
Perhaps the history of FH is able to contribute to a better understanding of that very important disease - which can save many lives, if adequately diagnosed and treated.
References
- Stefanutti C, et al. (2017) Toward an international consensus-Integrating lipoprotein apheresis and new lipid-lowering drugs. J Clin Lipidol. 11: 858-871. [PubMed.]
- Arnett D, et al. (2019) ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease. J Am Coll Cardiol. 140: e596–e646. [Ref.]
- Da Vinci IML, Anatomia D, Foglio B. (1901) W 191Royal Library, Windsor Castle. Published by Teodoro Sabachnikoff, transcribed and annotated by Giovanni Piumati and translated in French. Turin, Italy, Roux and Vi Arengo Editors M DCCCC I. The Queen's Special Permission and Dedicated to the Memoir of Her Most Gracious Majesty. [Ref.]
- Haller, Albrecht von. (1755) Opuscula Pathologica partim recusa partim inedita; quibus sectiones cadaverum morbosorum potissimum continentur. Accedunt experimenta de respiratione, quarta parte aucta. Neapoli, ex typographia Benedicti Gessari. 12: 352. [Ref.]
- Joseph R. (1978) 'Carl Rokitansky: A Reassessment of the Hematohumoral Theory of Disease.' "Bulletin of the History of Medicine." 52: 183-199. [Ref.]
- Kumar DR, Hanlin E, Glurich I, Mazza JJ, Yale SH. (2010) Virchow’s Contribution to the Understanding of Thrombosis and Cellular Biology. Clin Med Res. 8(3-4): 168-172. [Ref.]
- Lehzen G, Knauss K. (1889) Über Xanthoma multiplex planum, tubersoum, mollusciforma. Virchows Arch. Path. Anat. 116: 85. [Ref.]
- Tourueaux. (1913) Rev. de chir. 47: 7-8. [Ref.]
- Harbitz F. (1925) Svulster inneholdende xanthomvæv. Norsk Magazin for Lægevidenskaben. 321. (1927) Tumors of tendor Sheats, joint capsules and multiple xanthomata. Arch Pathol and Lab Med. 4: 507. [Ref.]
- Hoessli H. (1914) Über Xanthom der Haut und Sehnen, Beitrag klein. Chir. 90: 168. [Ref.]
- Török L. (1993) De la nature des xanthomes avec quelques remarques critiques sur la notion des tumeurs. Ann. Dermatol. Syph. 4: 1109. [Ref.]
- Müller C. (1939) Angina pectoris in heredary xanthomatosis. Arch Int Med. 64: 675. [Ref.]