>Corresponding Author : Kurt Widhalm
>Article Type : Research Article
>Volume : 3 | Issue : 4
>Received Date : 6 May, 2023
>Accepted Date : 1 June, 2023
>Published Date : 25 June, 2023
>DOI : https://doi.org/10.54289/JCRMH2300120
>Citation : Abdurrahman S, Olubunmi A, Gadzama D, Kefas IB, Dominguez J, et al. (2023) Knowledge, Perceived Risk, and Willingness for Vaccine Uptake of COVID 19 Among Primary Health Care Workers in Abuja, Nigeria. J Case Rep Med Hist 3(4): doi https://doi.org/10.54289/JCRMH2300120
>Copyright : © 2023 Abdurrahman S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Research Article | Open Access
1Public Health Department, Health and Human Services Secretariat, FCTA, Abuja
2Department of Community Medicine, Jos University Teaching Hospital Jos, Plateau State
3Institutd'Investigació Germans TriasiPujol; CIBER Enfermedades Respiratorias, Instituto de Salud Carlos III; and Genetics and Microbiology Department, Autonomous University of Barcelona (Barcelona, Spain)"
4Liverpool school of Tropical Medicine, Liverpool, United Kingdom
*Corresponding author: Kefas IB, Department of Community Medicine, Jos University Teaching Hospital Jos, Plateau State
Abstract
COVID 19 is a highly contagious disease, and health care workers are especially vulnerable. The novel virus has continued to wreak havoc in various countries around the world, particularly among the unvaccinated population. The study aimed to assess health workers' knowledge, risk perception, and willingness to receive the COVID 19 vaccine. This study utilized a cross-sectional design carried out among Primary Health Care Workers in the Federal Capital Territory (FCT) Abuja. A two-stage sampling technique was used to recruit 284 participants for the study. We adapted the Extended Parallel Process Model questionnaire to determine respondents’ knowledge, risk perception, and willingness to COVID 19 vaccine uptake. Data were analysed using SPSS version 23, and statistical significance was set at p<0.005. The average age of the study participants was 36 years. The study revealed, slightly more than half 167(58.8%) of respondents have a good knowledge of COVID 19. The relationship between sex and knowledge of coronavirus disease was statistically significant (p = 0.014). Most of respondents 260 (91.5%) were aware of the coronavirus vaccine. The majority of the respondents reported a lack of trust in government 140 (49.3%) and religion 33 (11.6%) as a reason for vaccine hesitancy. In our study, we found that HCWs' knowledge of COVID 19 was suboptimal, and their risk perception was low. Though vaccine willingness was high, vaccine hesitancy was primarily due to a lack of trust in the government.
Keywords: Risk Perception; COVID 19; Vaccine Uptake; Hcws
Abbreviations: HCW: Health Care Workers, FCT: Federal Capital Territory, AC: Area Councils, PHCB: Primary Health Care Board, SPSS: Statistical Package for Social Sciences, FCTHERC: FCTA Health And Research Ethics Committee
Introduction
Novel Coronavirus or COVID 19 is a new strain of viruses that is highly infectious and can infect humans causing life-threatening diseases [1,2]. COVID 19 is a public health emergency that has caused significant morbidity and mortality globally [3-5]. As of September 2021, an estimated 218 million cases of COVID 19 have been confirmed with more than 4.5 million deaths [4]. The African region is the least affected by the virus with an estimated 5.6 million confirmed cases [4]. This may be due to unclear epidemiological differences. COVID 19 has significantly interrupted both preventive and curative services, has contributed to a global economic recession with a looming food crisis, and has adversely affected the mental health and wellbeing of individuals and communities, especially in developing countries [6]. It has continued to cause devastating epidemics in the different countries of the world, especially among the unvaccinated population. Several efforts were put in place to prevent the spread of the virus. This includes the non-pharmaceutical measures of hand washing, or hand sanitizing with alcohol-based sanitizers, correct cough etiquette, avoidance of handshaking, wearing of facemask, and observing social distance. These countermeasures were remarkable and their effectiveness and success depend on knowledge and the risk perception of COVID 19 [7,8].
Health care workers (HCWs) clearly show increased vulnerability as they respond to patients during this COVID 19 global pandemic. HCWs had increased exposure to COVID 19 viral pathogen, long working hours, psychological distress, fatigue, occupational burnout and stigma, and physical violence [9]. There has been an increasing tension among healthcare workers proportional to the rise in figures of COVID-19 cases and mortality [10]. Frontline health care workers having more direct contact with disease patients in departments like the emergency department, intensive care unit, and infectious disease were found in a study to be at higher risk of covid-19 infection than administrative staff. These were found to show greater levels of fear, anxiety, depression, and psychological disorder than administrative staff [11].
The protection measures such as non-pharmaceutical protocols and lockdown taken by governments to contain the spread of the disease, although deemed necessary, have not significantly improved control of the pandemic [6]. Safe and effective vaccines are a critical tool to control the COVID 19 pandemic, and these vaccines have resulted in control of the epidemic, especially in developed countries where the coverage is significant especially for the vulnerable population. Estimated over 5 billion doses of the vaccine have been administered worldwide [7].
To introduce and install effective control measures, knowing basic hygiene principles and modes of disease transmission, and vaccination is important. To achieve ultimate success against the ongoing encounter against COVID-19, the uptake of the COVID 19 vaccines must be given a priority, Therefore, understanding the knowledge, risk perception, and willingness for vaccine uptake of COVID 19 among health workers is vital to achieving success [12].
Materials and methods
Study settings, design, and sample size
This was a cross-sectional study carried out from March 2021 to April 2021 in Federal Capital Territory. Federal capital territory (FCT), being the seat of the government of an emerging national economy, experiences an influx of people from diverse backgrounds. The estimated total population is 5,338,550 with a landmass of 1769km2.It has 6 Area Councils (AC) and 62 political wards [13].
The indigenes are mainly subsistence farmers and the major food crops include yam, maize, guinea corn, beans, and millet. Fishing activities are also prominent among the Bassa people and villagers along the rivers of Usma, Jabi, and Gurara. Pottery, wood, and craftwork are also the notable occupation of the people of the territory, especially the Gbagyis [14].
FCT operates a 3-tier health system of primary, secondary, and tertiary levels of care that spread over rural and urban areas. There are 754 accredited health facilities made up of 500 private health facilities and 254 public health facilities. The 254 public health facilities are disaggregated into 237 primary health facilities, 14 secondary health facilities, and 3 tertiary hospitals which are the National Hospital located in the Central Business Area of Abuja Municipal Area Council,
Federal Medical Centre (formerly Federal University of Abuja Teaching Hospital located in Gwagwalada Area Council. The three tertiary hospitals are owned and funded by the Federal Government, while the secondary facilities are managed by the Hospitals Staff Hospital) located at Airport Road and Management Board (HMB), and the PHC facilitiesare managed by the FCT Primary Health Care Board (PHCB). The private health facilities consist of hospitals, maternity homes, faith-based hospitals and clinics, diagnostic centers, and pharmacies. The private sector provides healthcare for a substantial proportion of the population [14].
The minimum sample size was calculated using the formula for a cross-sectional study. The significant level was placed at a 95% confidence interval, power of 80% using prevalence from a similar previous study [15].
Study population and sampling techniques
The study population consisted of consenting Primary Healthcare workers 18 years and above, residing and working in the FCT for at least six months were recruited into the study.
A two-stage sampling technique was used to select the study population. Two area councils were selected out of the six area councils in the FCT using the simple random sampling technique. The list of all the facilities and the health workers in each of the facilities were obtained as a frame for the two area councils. A proportion to size sampling technique was used to select the number of respondents in each facility.
Four staff of the primary health care board, two doctors, and four nurses from the facilities had 3 hours of daily training sessions for two days as research assistants on the study protocol and questionnaire conducted by the principal researcher. Written informed consent was sought and obtained from each eligible participant, and a semi-structuredinterviewer-administeredquestionnaire was used to collect information from all participants that fulfilled the inclusion criteria and gave consent.
Study instrument and data collection
A semi-structured interviewer-administered questionnaire adapted from the Extended Parallel Process Model based on risk perception assessments of other infectious diseases was used [16,17]. The questionnaire was pretested among 10% of the total sample size in a PHC facility in Karu LGA Information was collected on sociodemographic, knowledge of COVID 19, Sources of information on COVID 19, and vaccine acceptability.
Knowledge of cervical cancer was assessed using 31- a point knowledge score. The respondents were asked a total of 31 questions on the knowledge that carried a total of 31 correct responses. Each correct response was given a score of 1 and wrong responses a score of 0. The points (questionnaires) included symptoms, prevention, early detection, and treatment of the disease. Participants with a summary score greater than or equal to the mean value were categorized as having "good knowledge" and those with a score less than the mean were categorized as having "poor knowledge.
Measurement of variables
The dependent variables were knowledge and risk perception while social, and demographic characteristics were independent.
Data analysis
All the data generated was entered and analyzed using the IBM Statistical Package for Social Sciences (SPSS) version 23. A p < 0.05 was considered statistically significant for all statistical tests. Mean scores and standard deviations were used to summarise the quantitative variables. Chi-square was done to describe associations between sociodemographic features and the knowledge of participants on COVID 19. Risk perception and source of information were presented in proportions and graphs.
Ethical consideration
Ethical approval for the study was obtained from the FCTA Health and Research Ethics Committee (FCTHERC). Written informed consent was obtained from each study participant. Respondents were free to withdraw anytime during the study if they so desired. The participants were assured of the confidentiality of their information. All methods were carried out in accordance with relevant guidelines and regulations.
Results
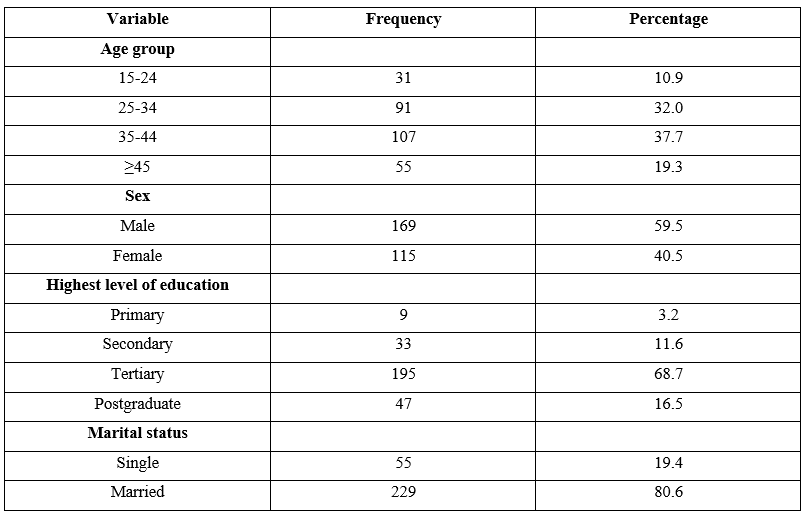
Table 1: Sociodemographic characteristics of respondents
Table 1: The mean age of the study respondents was 36 years. The age of the respondents was from 18 to 63 years old and it was distributed into 5 categories as follows; 15-24 years old 31(10.9%), 25 to 34 years 91(32.0%), 35 to 44 years 107(37.7%), and ≥45 55(19.3%). More than half of the respondents were males 169(59.5%), while 115(40.5%) were females. The majority of the respondents were having tertiary education. Most of the respondents were married 229(80.6%).

Table 2: Knowledge of coronavirus disease among respondents
Table 2: The mean knowledge score of respondents was 14.40 ± 4.40. Table 2demonstrated that slightly greater than half of the study respondents 167(58.8) had good knowledge of coronavirus disease.
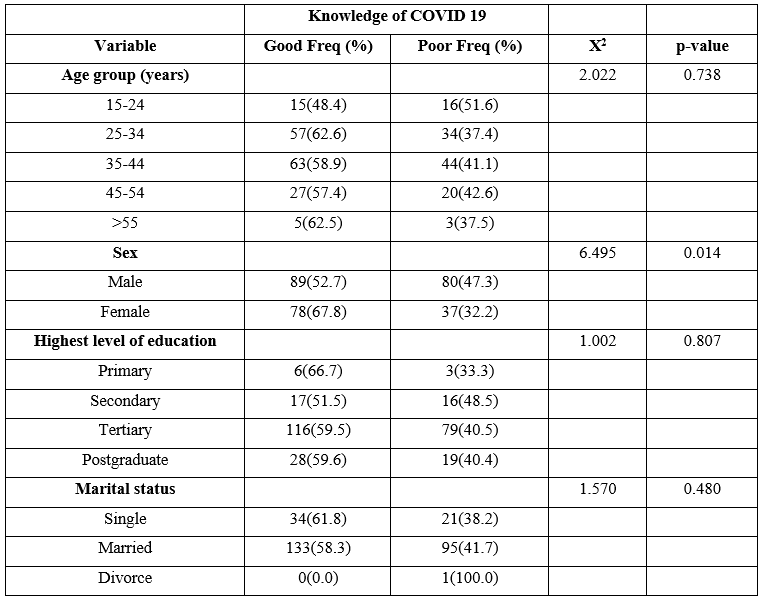
Table 3: Factors associated with knowledge of Coronavirus disease among healthcare workers
Table 3: There was no significant difference in the knowledge of coronavirus disease between the different age groups (p > 0.738). However, more than half of the respondents in the different age groups had good knowledge of coronavirus disease except those in the younger age group15 - 24 years. There was a statistically significant association between sex and knowledge of coronavirus disease (p = 0.014).
There was no significant association between level of education and knowledge of coronavirus disease. There was no significant difference (p = 0.480) between single, married, and divorced.
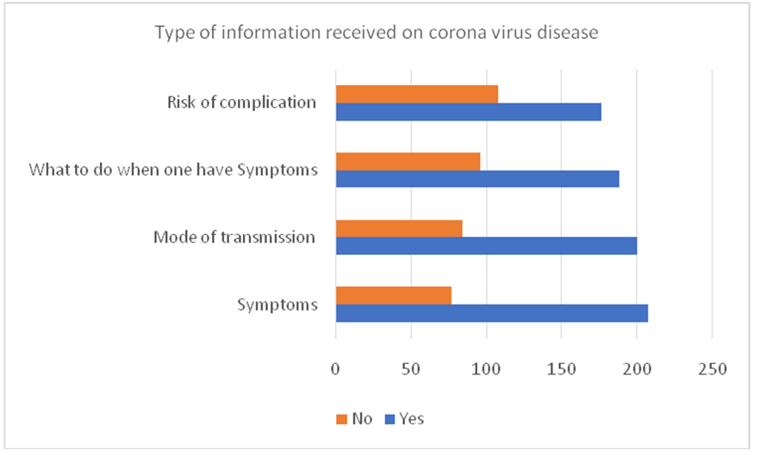
Figure 1: Different information received on coronavirus disease
Fig. 1: Most of the respondents reported that the most frequent information they received was on how to protect themselves 258(90.8%), this was followed by information on the disease symptoms 207(72.9%), Mode of transmission 200(70.4%), what to do when one has the disease 188(66.2%) and risk of complication of the disease 176(62.0%).
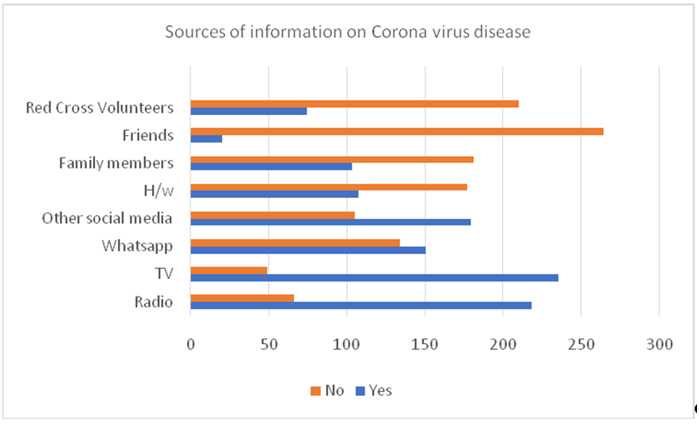
Figure 2: Sources of information on coronavirus disease
Fig. 2: Respondent’s source of information on coronavirus disease was the television 235(82.7%), radio 218(76.8%), and WhatsApp 150(52.2%). The least source of information was through friends 107(37.7%). Only about half of the respondents got their information from health workers
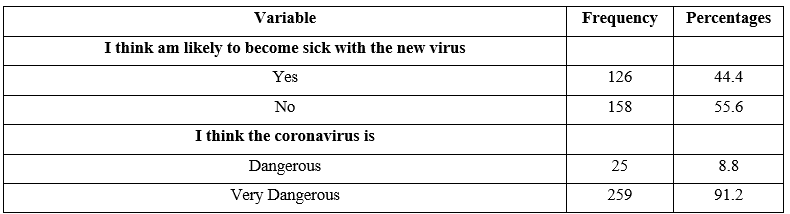
Table 4: Risk perception of coronavirus disease among health workers
Table 4: The majority of the health workers perceived themselves as not likely to become sick with coronavirus 158(55.6%). Most of the health healthcare workers believe that the coronavirus disease was very dangerous 259(91.2%) and 25(8.8%) believe that the disease was dangerous but none of the respondents reported that coronavirus disease was not dangerous.
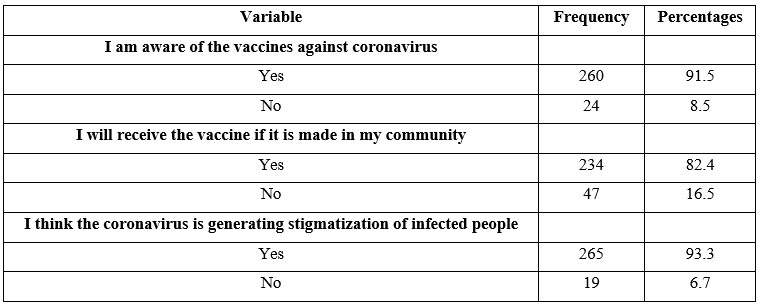
Table 5: Awareness and willingness for COVID 19 vaccine uptake among health workers
Table 5: Most of the health workers were aware of the coronavirus vaccine 260(91.5%) with a majority of the respondents 234(82.4%) willing to take the coronavirus vaccine if it is made available in the community.
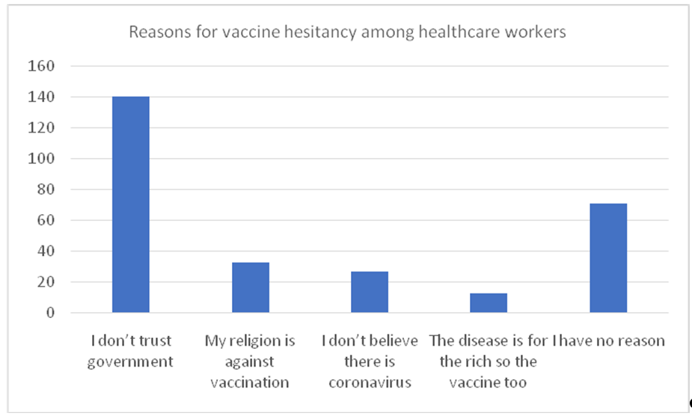
Figure 3: Reason for vaccine hesitancy among healthcare workers
Fig. 3: The majority of the respondents reported the reason for vaccine hesitancy to be a lack of trust in the government 140(49.3%). Other reasons for the vaccine hesitancy were religion 33(11.6%), don't believe in the existence of coronavirus 27(9.5%), and the disease is main for the rich 13(4.6%). Others 71(25.0%) did not give any reason for hesitancy but may not avail themselves to receive the vaccine.
Discussion
This study shows that more than of the respondents have good knowledge of coronavirus diseases. This was higher than the finding of a study done among the general population in Kebbi state where only about a third had good knowledge toward control of COVID 19 [8]. A study done amount University students in Japan reported good knowledge scores in most of the studied population compared to our study [7]. This may be because the pandemic impeded directly on their daily lives and academic activities compared to other adults and may have compelled them to acquire some knowledge about the disease. In addition, the provision of guidelines and protocol for proper conduct during the pandemic may have influenced their knowledge. Another study was done among the Iranian population and also revealed that the majority have good knowledge of COVID 19 [12]. The finding in this study may reflect increased exposure to information on COVID 19 from governments and media. Almost half of the respondents in this study had poor knowledge of the disease. This was worrisome as this study was carried out among health care workers who are expected to have adequate and correct knowledge of the virus and also serve as a source of information for the general population, this had great implications for COVID 19 control.
Our study did not find a significant association between knowledge of coronavirus disease and age groups. In contrast, other studies reported an association between good knowledge and age greater than 30 years [1,8,18]. This may be since the older persons are mostly those that are married and are quick to take actions that will protect them and their families. In addition, at this age, many of the respondents are already involved in COVID 19 campaigns about either prevention or treatment of the infected people. In this study, we found that the male gender was associated with good knowledge of coronavirus disease. However, this was inconsistent with the finding of a study carried out in Japan that females had more basic knowledge and explained the information more correctly than males, which agrees with previous studies in other countries showing that females have higher knowledge about COVID-19 and a proper attitude [7]. Another study done in Northern Nigeria reported no significant association between gender and knowledge of coronavirus disease [8]. Based on these findings, to improve health education support programs regarding the knowledge about COVID-19, more targeted approaches for certain demographic characteristics such as gender is required.
In this study, level of education was not associated with knowledge of coronavirus disease. This was not consistent with a study done in Syria that revealed that a tertiary level of education was associated with knowledge of coronavirus disease [7,12]. The finding in this study was that the majority of the respondents have a higher level of education and are health care workers. Differences in methodology and study population may have also contributed to the disparity.
We find that the most frequent information received by health workers was on the symptoms of COVID 19 and the mode of transmission of the virus. The leas information received by the HCWs was at risk of complication. This was because the COVID 19 was not fully understood and information on the complication was evolving. The major source of information on coronavirus disease reported was the television and radio. A similar finding was reported in a study carried out among HCWs in Makerere [18]. This suggests that these channels of communication should be utilized in planning and implementing health promotion and risk communication in the population.
Less than half of the respondents perceived themselves as likely to be sick with the virus and all respondents believe that the coronavirus was dangerous or very dangerous. This was similar to findings reported in studies done in Ethiopia and Iran where most of the respondents have a high-risk perception [2,19]. Other studies carried out in India and Gondar city reported lower risk perception [20,21]. This might be due to the differences in the study population, methodology, data, and level of spread of the virus across countries and communities. It may also be accounted for by the level of access to information, level of knowledge, and risk communication of the local authorities Also, risk perceptions can influence health-related behaviors and can play a substantial role in disease control as individuals are likely to adhere to preventive measures.
In this study, a majority (>90%) of the HCWs were aware of the vaccine against coronavirus and most of the respondents were willing to receive the vaccine if it is made available. The finding was consistent with a study conducted in seven European countries from Denmark, France, Germany, Italy, Portugal, the Netherlands, and the UK stating that they would be willing to get vaccinated against COVID-19 if a vaccine would be available [22]. A study done in Australia reported less proportion of participants willing to receive the vaccine [23]. Getting HCWs vaccinated is a critical preventive measure in light of an increased COVID 19 risk of HCWs. Most of the HCWs reported a lack of trust in the government and religion as the reason for vaccine hesitancy. This has implications for the COVID vaccine uptake since the HCWs at the community level are an integral part of the strategy to achieve coverage needed for herd immunity. This was challenging against the backdrop of poor vaccine compliance and coverage in Nigeria.
Limitation
Our study considers only HCWs at the primary health care facilities and this may not reflect the knowledge of HCWs in the FCT. The close-ended question on vaccine hesitancy may have limited individuals' responses. There is a need for a community-based study with a qualitative component to explore willingness for COVID 19 vaccine uptake in the context of the community.
Conclusion
The study highlighted that knowledge of COVID 19 was sub-optimal among HCWs. The main source of information on COVID 19 was news media such as televisions and radio. Risk perception among HCWs was low. However, the willingness for COVID 19 vaccine uptake was high. There is a need to continue to improve the knowledge of HWCs on COVID 19 and implement strategies that consider their belief system and perception in developing control measures.
Consent for publication: Not applicable
Availability of data: The dataset generated or analyzed during this study is included in this published article and its supplementary information files uploaded.
Competing interests: The authors declared no competing interest
Sources of support: The research work is completely sponsored by the authors.
Authors’ contributions: AS, JD, LEC, and OA contributed to the conceptualization and design. GD acquired articles for review, abstracted findings to tables, and contributed to analysis and interpretation. KIB carried out data analysis.
All the authors participated in the review and critique process and revised it critically for intellectual content. All the authors read and approved the final manuscript.
Acknowledgment
We are grateful to Institutd' Investigació Germans Triasi Pujol; CIBER Enfermedades Respiratorias, Instituto de Salud Carlos III; and Genetics and Microbiology Department, Autonomous University of Barcelona (Barcelona, Spain)" and FCT Public Health Department which provided technical directives and guidance for the COVID 19 response in the territory.
References
- Labban L, Thallaj N, Labban A. (2020) Assessing the Level of Awareness and Knowledge of COVID 19 Pandemicamong Syrians. Arch Med. 12(3): 8. [Ref.]
-
Tadese M, Haile AB, Moltot T, Silesh M. (2021)
Perceived Risk of COVID-19 and Related Factors Among University Students in Ethiopia During School Reopening
. Infect Drug Resist. 14: 953-961. [PubMed.] - WHO. (2021) Acceptance of available traditional vaccine supply with reduced shelf-life. Interim Guid. 1-5. [Ref.]
- WHO. WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. [Ref.]
- WHO. (2021) R&D Blueprint and COVID-19. [Ref.]
- WHO. (2020) Best practices for developing surveys and questionnaires on the impacts of COVID-19 on fisheries and aquaculture. Food and Agriculture Organization of the United Nations. [Ref.]
- Hatabu A, Mao X, Zhou Y, Kawashita N, Wen Z, et al. (2020) Knowledge, attitudes, and practices toward COVID-19 among university students in Japan and associated factors: An online cross-sectional survey. PLoS One. 15(12): e0244350. [Ref.]
- Habib MA, Dayyab FM, Iliyasu G, Habib AG. (2021) Knowledge, attitude, and practice survey of COVID-19 pandemic in Northern Nigeria. PLoS One. 16(1). [Ref.]
- Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. (2020) Coronavirus Disease-2019: Knowledge, Attitude, and Practices of Health Care Workers at Makerere University Teaching Hospitals, Uganda. Front Public Heal. 8: 181. [Ref.] [PubMed.]
- Ahmed AMK, Ojo OY, Imhonopi GB, Oladeji FO, Oyesola OA, et al. (2020) Knowledge, perceptions, and safety practices of COVID-19 infection among healthcare workers in a tertiary health institution, Southwest, Nigeria. Int J Community Med Public Heal. 7(12): 4697-705. [Ref.]
- Gross JV, Mohren J, Erren TC. (2021) Original research: COVID-19 and healthcare workers: a rapid systematic review into risks and preventive measures. BMJ Open. 11(1). [Ref.]
- Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. (2020) Title: Knowledge, Attitude and Practice toward the Novel Coronavirus (COVID-19) Outbreak: A Population-Based Survey in Iran. E- pub. [Ref.]
- Elleh N. (2001) Abuja: the single most ambitious urban design project of the 20th century. New World Encycl. 97. [Ref.]
- Federal Capital Development Agency. Federal Capital Territory (Nigeria). [Ref.]
- Charan J, Biswas T. (2013) How to Calculate Sample Size for Different Study Designs in Medical Research? Indian J Psychol Med. 35(2): 121. [Ref.]
- Popova L. (2012) Regular Articles The Extended Parallel Process Model: Illuminating the Gaps in Research. Heal Educ Behav. 39(4): 455-473. [PubMed.]
- Jahangiry L, Sarbakh P, Reihani P, Samei S, Sohrabi Z, et al. (2020) Developing and validating the risk perceptions questionnaire for COVID-19 (Risk Precept COVID-19): an application of the extended parallel process model Research Square. [Ref.]
- Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. (2020) Coronavirus Disease-2019: Knowledge, Attitude, and Practices of Health Care Workers at Makerere University Teaching Hospitals, Uganda. Front Public Heal. 8: 181. [PubMed.]
- Honarvar B, Lankarani KB, Kharmandar A, Shaygani F, Zahedroozgar M, et al. (2020) Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. Int J Public Health. 65(6): 731-739. [Ref.]
- Kuang J, Ashraf S, Das U, Bicchieri C. (2020) Awareness, Risk Perception, and Stress during the COVID-19 Pandemic in Communities of Tamil Nadu, India. Int J Environ Res Public Health. 17(19): 7177. [PubMed.]
- Kabito GG, Alemayehu M, Mekonnen TH, Wami SD, Azanaw J, et al. (2020) Community's perceived high risk of coronavirus infections during the early phase of epidemics are significantly influenced by socio-demographic background, in Gondar City, Northwest Ethiopia: A cross-sectional -study. PLoS One. 15(11): e0242654. [Ref.]
- Neumann-Böhme S, Varghese NE, Sabat I, Barros PP, Brouwer W, et al. (2020) Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur J Heal Econ. 21(7): 977-982. [PubMed.]
- Dodd RH, Cvejic E, Bonner C, Pickles K, McCaffery KJ, et al. (2021) Willingness to vaccinate against COVID-19 in Australia. Lancet Infect Dis. 21(3): 318-319. [Ref.]