>Corresponding Author : Nalini M. Rajamannan
>Article Type : Case Report
>Volume : 3 | Issue : 8
>Received Date : 10 Nov, 2023
>Accepted Date : 20 Nov, 2023
>Published Date : 25 Nov, 2023
>DOI : https://doi.org/10.54289/JCRMH2300137
>Citation : Rajamannan NM. (2023) A Tale of Two Rings: The Need for Informed Consent. J Case Rep Med Hist 3(8): doi https://doi.org/10.54289/JCRMH2300137
>Copyright : © 2023 Rajamannan NM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access
1Most Sacred Heart of Jesus Cardiovascular and Valvular Institute, Chicago IL
2Division of Biochemistry and Molecular Biology, Visiting Scientist, Mayo Clinic College of Medicine, Rochester MN
*Corresponding author: Nalini M. Rajamannan, Most Sacred Heart of Jesus Cardiovascular and Valvular Institute, Chicago IL and Division of Biochemistry and Molecular Biology, Visiting Scientist, Mayo Clinic College of Medicine, Rochester MN
Brief Summary
Over the past 85 years, the mission of the FDA’s Center for Device and Radiologic Health has been to provide safe medical devices for the US consumer, and to adapt the regulatory standards to meet the needs of the rapidly evolving medical device industry. This brief report is the historical account of two investigational devices dating back to 2006, the devices never receiving FDA approval for use in patients during a clinical trial, and the patients never received informed consent.
Abbreviations: DHF: Design History File, SEC: Security Exchange Commission, V. Fib: Ventricular Fibrillation, MC: Mayo Clinic
Brief Report
Myxomatous mitral valve disease is the most common cause of severe mitral regurgitation, in the United States and Europe. This brief report will outline the regulatory history of the device, and the outcomes of two patients who underwent safety and efficacy testing of a new annuloplasty prototype ring medical device [1], for myxomatous mitral valve disease prior to the manufacturer’s marketing launch on the US market.
Safety and Efficacy Study
From 2006-2007 [2,3], patients received a newly invented, patent pending [4] annuloplasty device model 5100, during a safety and efficacy study, for the design history file (DHF) [5,6]. Prior to open heart surgery for myxomatous mitral valve disease, the investigator, who is also the inventor of the investigational device [7,8] asked patients to sign an IRB approved [9,10] registry to follow their clinical course after open heart surgery [9-14]. The registry did not specifically inform the patients that they were receiving a device to test for safety and efficacy prior to sales on the US market, nor did it inform the patients that the surgeon received royalties as the inventor of the annuloplasty ring [9,10].
After ten months of validation testing and modifications, the manufacturer formally released the modified second version of the device to the US market in the first quarter of 2007, as per reporting by the manufacturer to the Security Exchange Commission (SEC) in the annual 10-k filings [5]. Furthermore, Edwards Lifesciences announced the US launch of the model 5100, at the Society of Thoracic Surgeons 2007 annual meeting [6]. The study results were used for 1) to maintain the evolution of the annuloplasty ring in the DHF, 2) to submit final design modifications to defend the US patent office in 2007 [4], 3) to publish the study in the Journal of Thoracic and Cardiovascular Surgery in 2008, and finally 4) to obtain FDA clearance for the 510(k) application submitted in 2008 and cleared in April 2009 [13].
Patient Outcomes In 2006
This historical case report provides data from two patients, who received the prototype test unit called the McCarthy Annuloplasty ring [3] to measure safety and efficacy, as compared to the predicate device, without informed consent. The first report is of a patient who received the device in April 2006, during the early initial implants. The patient developed progressive symptoms of shortness of breath over the next ten months, after receiving newly invented prototype Model 5100 ring for mitral valve prolapse, and the use of an experimental surgical protocol entitled the modified Alfieri stitch [4,11].
In January 2007, this patient underwent diagnostic imaging studies, which demonstrated severe mitral stenosis with a mean gradient of 12 mmHg across the mitral valve, and a mitral valve area of 1.0 cm2. The patient’s symptomatic severe mitral stenosis resulted in a Horner’s syndrome with secondary laryngeal nerve compression from her severe left atrial enlargement. The patient underwent a second open-heart surgery in May 2007, to remove the ring and replace the mitral valve with a mechanical St. Jude mitral valve, implantation of a tricuspid annuloplasty ring, model 4625, and receive a second MAZE procedure at an outside institution. Pathology was reviewed at an outside institution, which demonstrated an intense inflammatory infiltrate, without rheumatic disease, and the Vicryl suture material placed in the anterior leaflet for the modified Alfieri Stitch technique [4,11].
Gross Pathology and Mitral Annuloplasty Ring
The gross pathology of the mitral valve removed during the second surgery demonstrated the mitral annuloplasty ring, model 5100, and the severe myxomatous anterior mitral valve leaflet as shown in Figure 1, Panel A. Figure 1, Panel B, demonstrates the atrial surface of the diseased valve leaflet and Figure 1, Panel C, demonstrates the ventricular surface of the valve leaflet. The valve was then sectioned to show the increase in the anterior valve leaflet thickness associated with the blue Vicryl stitch used for the repair technique, known as a modified Alfieri Stitch [14], as shown in Figure 1, Panel D. The posterior leaflet photographed in Figure 1, Panel D, demonstrated no change in the leaflet thickness and no suture material. Figure 1, Panel E, demonstrates a graphic illustration of the modified Alfieri stitch. Figure 1, Panel F, demonstrates the Hematoxylin and Eosin stain of the suture and inflammatory response surrounding the suture material. The progressive thickening of the anterior leaflet secondary to the sutured leaflet and acute inflammatory response caused a rapidly progressive case of severe symptomatic mitral stenosis and chronic NYHA Class II heart failure.
A second patient suffered a ventricular fibrillation (V. Fib) cardiac arrest treated with amiodarone and cardioversion in the operating room, after coming off bypass, and a second V Fib arrest at 12:58 pm requiring cardioversion. At 1:13 pm a diagnostic ECG was obtained on November 6, 2006, 30 minutes after the patient left the operating room, which demonstrated a posterior lateral myocardial infarction during the immediate peri-operative period as shown in Figure 2, Panel A. The myocardial infarction was not treated after, as per 2004 ACC/AHA guidelines [15]; the infarct progressed resulting in a significant and permanent loss of myocardial function.
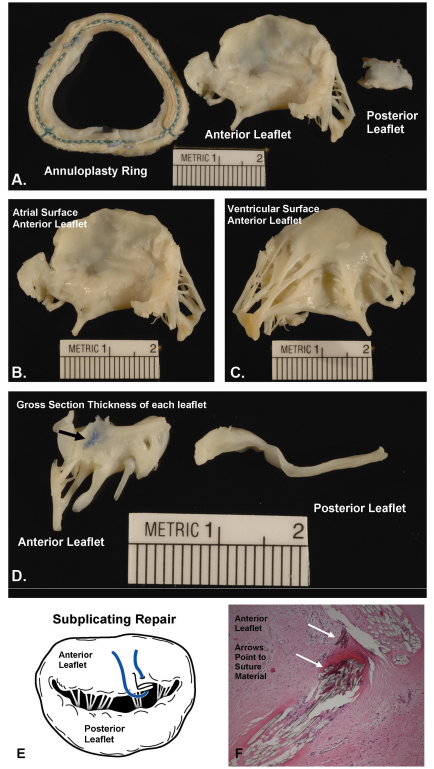
Figure 1. Photographs of the Gross Pathology from the Surgically Removed Mitral Valve Leaflet.
Panel A. Mitral Annuloplasty Ring and Myxomatous Mitral Valve Anterior Leaflet
Panel B. Atrial Surface of the Anterior Mitral Valve Leaflet
Panel C. Ventricular Surface of the Anterior Mitral Valve Leaflet
Panel D. Cross section through the Mitral Valve Leaflet demonstrating the Blue Vicryl Stitch
Panel E. Graphic Illustration of the Modified Alfieri Stitch
Panel F. H and E stain of the anterior leaflet, Arrow points to suture material and inflammatory cells(20x Magnification)
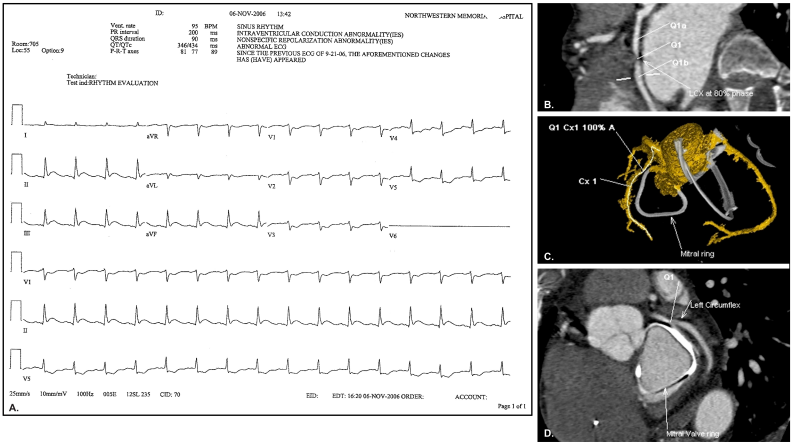
Figure 2. ECG from Patient 2 and CT left circumflex artery and the device compressing the artery, see video in the supplementary files.
Panel A. ECG Immediately post-op demonstrating evolving posterior-lateral myocardial infarction.
Panel B. Coronal CT view of the left circumflex artery
Panel C. Annuloplasty ring
Panel D. CT angiography demonstrating minimal flow through the left circumflex artery.
United States Senate Finance and Judiciary Committee Investigations
Between December 2008-2014, the Honorable Senator Charles Grassley(IA) led several investigations requesting documents surrounding the testing of the device without FDA authorization and without patient consent [7,14,19]. The FDA Congressional letter to the Senate Finance Committee confirmed that the Myxo ETlogix, the second version of the model 5100, is confirmed investigational as of March 2009 [7].
FDA Compliance Investigation: Myxo ETlogix device Model 5100 classified under
Investigational Device Exemption
In July 2008, patient one reported the adverse outcome to the FDA MAUDE database and received an email from the FDA confirming that model 5100 was not approved. In December 2008, the device was removed from the US market during a voluntary FDA recall [16]. The manufacturer was allowed by the FDA, to submit a first time 510(k) application, based on the results of the safety and efficacy study [2,3,7]. Model 5100 was eventually cleared under a new 510(k) [13], but given new name, D’ETLogix, to comply with the 510(k) requirements to avoid misbranding [8,17]. This new name includes the indication for any etiology of mitral valve disease as outlined in the 1997 guidelines, when to submit a new 510(k) [8,17]. The first two versions of the Model 5100 ring, the Myxo ETLogix ring never received FDA approval due to misbranding violations, as reported in the FDA Warning letter, [18-20] see Figure 3, Panel A and B.
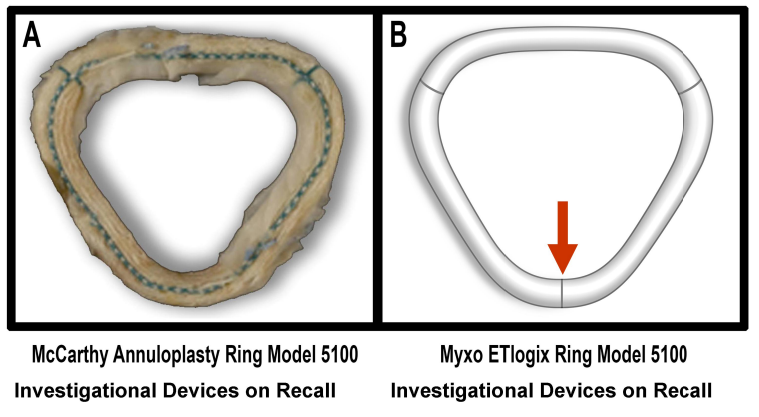
Figure 3.
Panel A, McCarthy Myxo Prototype, March 6, 2006- November 20, 2006, No FDA IDE, or Registration
Panel B, Myxo ETlogix Ring, November 20, 2006-December 5, 2008, Addition of marker to delineate front from back of the ring, No FDA IDE, or Registration, Myxo ETlogix classified as investigational as of today according to FDA’s compliance review for misbranding indications for use.
The FDA’s compliance investigation determined, 1) the device did constitute major changes, and 2) that patients need to informed they were enrolled in the experimental surgeries [19,21].
On July 16, 2009, the Congressional office for the FDA confirmed that the Myxo ETlogix model 5100 meets criteria for an Investigational Device Exemption [22]. The FDA determination would require an IRB consent with more information for the patients, than the signed outcomes registry that did not include information regarding the safety and efficacy testing. This FDA regulatory law is also stated in the IRB member handbook for Northwestern University at the time of the safety and efficacy testing for model 5100, which requires the institution, the investigator, and the sponsor to inform the patients of the implantation of the significant risk annuloplasty device. IRB Handbook provided to the Senate Finance Committee.
In 2011, the Director for CDRH, Dr. Jeffrey Shuren further confirmed this determination that there were two annuloplasty rings the IMR [22] and the Myxo ETlogix [3] which are currently classified as experimental prior to the April 2009 510(k) clearance [11,12]. Finally, in December 2018, the FDA released the August 8, 2008 inspection of Northwestern University’s Human Subject
Protections office, confirming two facts: 1) No FDA approval was filed in the database, and 2) The IRB terminated the data registry for non-compliance in July 2007, requiring all surgical testing to end [22-27]. The study continued until November 2007. As of 2023, the FDA Maude database injuries, deaths etc. for the investigational devices, as retrieved by Device Events for this report, see Figure 4.
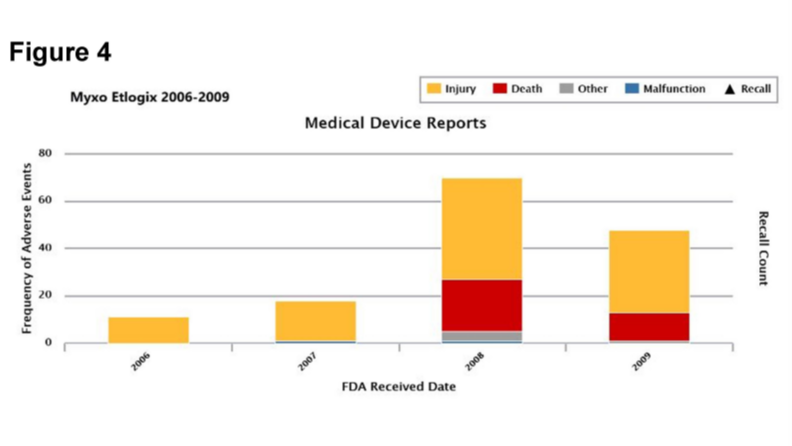
Figure 4.
FDA Maude database: Adverse Events for Myxo ETlogix Ring, 2006-2009
Permission to reproduce CEO Device Events, Madris Kinnard, CEO Device Events
Former FDA, CDRH, Public Health Analyst, Center for Devices, http://www.deviceevents.com.
Conclusion
Mitral annuloplasty rings are classified as Significant Risk Class II devices. Device manufacturers are required to maintain a design history file to historically document the evolving technology of predicate devices, and to determine the safety and efficacy comparing the newer generation of medical devices to the predicate device, prior to sales on the US market. Historically, the FDA clarified that these safety and efficacy studies, to support marketing applications, fall under the laws, which protect human subjects (21 CFR title 50.3).
The tale of two rings, includes to date, 667 Myxo ETlogix annuloplasty units, model 5100 have been implanted in patients during open-heart surgery without informed consent of the investigational nature of the device, nor have the patients been informed they received an experimental device by Northwestern. These case reports will help unsuspecting physicians to identify their patients who were involved in a safety and efficacy study to first, inform their patients that they received the experimental IDE devices, as confirmed in Congressional and Federal Investigations; second, to recognize the complex adverse outcomes surrounding the design of this device and surgical technique, and third, to provide health care necessary for their participation in the safety and efficacy clinical testing, and finally to report any ongoing adverse events for these unsuspecting patients to the FDA.
Acknowledgements
The author removed participation in referring patients to the study in the May 2007, when patient one revealed that the IRB she signed was an atrial fibrillation database, and that there was no informed consent provide to receive the McCarthy annuloplasty ring model 5100, and informed the University and the board of trustees for Northwestern University. Funding from NIH/ARRA supported the author’s salary 1R01HL085591-01A1 at the time of analysis. The use of human tissue was approved by the Human Subject Protection Offices, at the Mayo Clinic (MC) (771-01). Tissue was collected at the time of surgery at the Cleveland Clinic. The patient provided consent to the Cleveland Clinic for the evaluation of the valve pathology. The author thanks Dr. William Edwards for the images of the mitral valve pathology from the department of Pathology at the Mayo Clinic, Rochester MN. The author thanks the Patients© who provided consent to release their medical data for this report
References
- Kaplan AV, Baim DS, Smith JJ, et al. (2004) Medical device development: from prototype to regulatory approval. Circulation. 109: 3068-3072. [PubMed.]
- McCarthy PM, Rajamannan NM, McGee EC, et al. Novel Surgical Approach to Myxomatous Mitral Valve Repair. Jctvs. [Ref.]
- AATS. (2007) Abstract 2007 AATS meeting 2007, retracted in 2021 by the AATS in 2021 for the inventor ethics violations. [Ref.]
- McCarthy PM. (2004) Annuloplasty Ring for Mitral Valve Prolapse. United States Patent and Trademark Office ECV 5785. [Ref.]
- Edwards L, Sciences. (2013) Security Exchange Commission Annual 2008 10-k Filing. Edgar Database Accessed on June 30. 133. [Ref.]
- Edwards L, Sciences. (2013) Edwards Lifesciences Highlights Newest Heart Valve Innovations at AATS 2007 New Study Results Demonstrate Efficacy of Edwards Myxo ETlogix Annuloplasty Ring. 2. [Ref.]
- Ireland J. (2009) FDA Assistant Commissoner for Legistlation Letter to Honorable Senator Grassley. [Ref.]
- FDA. (1997) Deciding When to Submit a 510(k) for a Change to an Existing Device (K97-1). FDA. [Ref.]
- Adams A. (2008) Office of Research Integrity Statement. Response. [Ref.]
- Ann K. Adams. (2008) Office of Research Integrity Statement Response. [Ref.]
- Shelton D, Grotto J. (2011) Patients at Heart of Medical Device Issue. Chicago Tribune. [Ref.]
- Grotto J, Shelton D. (2011) Heart-Valve Rings Slip through FDA Loophole. Chicago Tribune. [Ref.]
- Li A. (2023) In Focus: Years after surgery, new documents renew patients’ malpractice claims against Northwestern Memorial doctor. [Ref.]
- (2014) Northwestern University's response to Senate Judiciary investigation. 6275. [Ref.]
- Antman EM, Anbe DT, Armstrong PW, et al. (2004) ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction--executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. [PubMed.]
- FDA, William C MacFarland. (2008) Edwards L, Sciences. recall documents. Department of health & Human services. [Ref.]
- FDA. (2013) Guidance for Annuloplasty Rings 510(k) Submissions) Final Guidance for Industry and FDA Staff. [Ref.]
- Maisel WH. (2009) Medical Devices Are Current Regulations Doing Enough For Patients? Testimony Maisel. [Ref.]
- (2008) Honorable Senator Charles Grassley, United States Senate Finance Committee [Ref.]
- Mussallem MA.FDA. (2010) Warning Letter. US Food and Drug Administration. [Ref.]
- Harrison. M (2008) Determination to Northwestern University submitted to United States Finance. FDA. [Ref.]
- Atonist V. (2008) Congressional Letter. FDA. Department of Health & Human Services. [Ref.]
- FDA FOIA (2018-9249) Establishment Inspection Report, Inspector Lisa Hayka. FDA. 7. [Ref.]
- Tasha O. (2018) Freedom of Information Act 2018-9249. Jessica Whitng. FDA. [Ref.]
- (2018) Freedom of Information Act 2018-9249, Jessica Whitng. Federal Termination Contract. FDA. [Ref.]
- Senate Finance Committee Communication. (2006) Myxologix Mitral Annuloplasty Ring. Edward Life Science. FDA. [Ref.]
- (2007) Mitral Annuloplasty Ring. Edward Life Science. FDA. [Ref.]