>Corresponding Author : Safaa Mhaber
>Article Type : Case Report
>Volume : 3 | Issue : 8
>Received Date : 14 Nov, 2023
>Accepted Date : 27 Nov, 2023
>Published Date : 02 Dec, 2023
>DOI : https://doi.org/10.54289/JCRMH2300138
>Citation : Mhaber S, Kabli AE, Mourabit S, Echchilali K, Moudatir M, et al. (2023) An Evans Syndrome Revealing a Renal Neoplasm. J Case Rep Med Hist 3(8): doi https://doi.org/10.54289/JCRMH2300138
>Copyright : © 2023 Mhaber S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access
1Resident Physician, Department of Internal Medicine, Ibno Rochd University Hospital, Casablanca, Morocco
2Professor in the Department of Internal Medicine at the Ibno Rochd University Hospital in Casablanca, Morocco
*Corresponding author: Safaa Mhaber, Resident Physician, Department of Internal Medicine, Ibno Rochd University Hospital, Casablanca, Morocco
Abstract
We present a rare case of Evans syndrome associated with clear cell renal cell carcinoma, in which the patient showed rapid restoration of blood cell count and durable complete remission of Evans syndrome after resection of the renal tumor. A thorough examination led to the diagnosis of Evans syndrome. We hypothesized that our patient's initial hematological manifestation was a paraneoplastic phenomenon associated with her underlying malignancy. This rare case illustrates the unique relationship between renal neoplasm and the development of paraneoplastic Evans syndrome.
Abbreviations: PNS: Paraneoplastic Syndromes
Introduction
Paraneoplastic syndromes (PNS) are defined by a set of clinical, radiological or biological signs associated with a neoplasia, irrespective of its location.
Cancer patients, particularly those at an advanced stage, may present with a variety of hematological manifestations, but Evans syndrome is a rare PNS in malignant solid tumors. We present a rare case of Evans syndrome revealing to clear cell renal cell carcinoma.
Case presentation
A 64-year-old female patient was diagnosed with Evans syndrome associating severe thrombocytopenia with 2000 platelets and autoimmune hemolytic anemia. Myelogram and BOM showed a rich hematopoietic marrow for her age; infectious and immunological workups were negative. Bolus corticosteroids were administered, followed by high-dose oral CTC, with good initial clinical and biological evolution. The evolution was marked by 2 episodes of relapse with corticodependence at 40 mg per day. A thoraco-abdomino-pelvic scanner was performed as part of the etiological work-up, showing a suspicious right renal mass. A total right nephrectomy was performed, with histological evidence of clear-cell renal cell carcinoma (figure 1). A paraneoplastic Evans syndrome was finally identified.
Azathioprine-based disease-modifying therapy was initiated, and the patient is currently in haematological remission after 12 months.
Discussion
Paraneoplastic syndromes (PNS) are a group of secondary manifestations associated with neoplasia, irrespective of its primary location or metastases. They are the consequence of aberrant hormone ectopic production, or an autoimmune reaction by the tumor that improves with effective treatment of the underlying cancer. They are not specific, but should be systematically investigated for cancer. It is difficult to determine their prevalence due to their rarity. according to the few studies carried out, their prevalence reaches 8% in cancer patients [1].
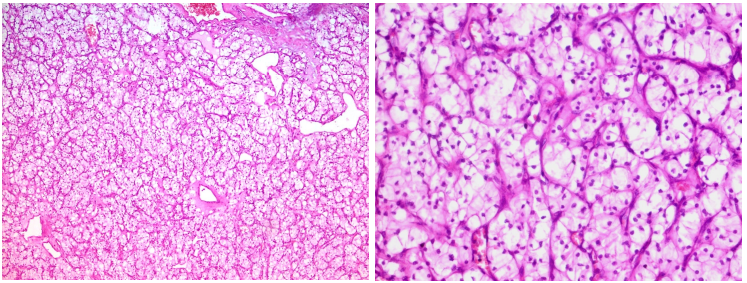
Figure 1.Histological images of a clear cell renal cell carcinoma. On the left, carcinomatous proliferation organized in nests with thin-walled vessel-rich stroma in the background [x100, under standard staining]. On the right, the cells are well limited, with clear optically empty cytoplasm and round nuclei without nucleoli (ISUP grade 1) [x400, under standard staining].
The first case of a combination of idiopathic thrombocytopenia purpura and autoimmune hemolytic anemia was described by Evan et al this clinically rare entity is referred to as Evans syndrome [2].
Autoimmune hematological diseases such as evans syndrome is the most common NPS in lymphoid neoplasms [3]; however, secondary Evans syndrome is a much rarer NPS in malignant solid tumors particularly in renal tumors [4]. A secretion of cytokines, hormones or peptides implies cross-immune reactivity between normal and malignant tissue is strongly suspected [5].
Our patient presents a rare case of Evans syndrome associated with clear cell renal cell carcinoma in which the patient showed rapid normalization of complete blood count and durable complete remission of Evans syndrome after tumor resection.
Conclusion
The possibility of a solid tumor should be considered in the presence of Evans syndrome. Internists, oncologists and hematologists should therefore be made more aware of Evans syndrome, so that they can take prompt action to recognize and diagnose malignant tumors earlier, for better diagnostic and therapeutic care and a better prognosis.
References
- Pelosof LC, Gerber DE. (2010) Paraneoplas:c syndromes: Anapproach to diagnosis and treatment. Mayo Clin Proc. 85: 838-854. [PubMed.]
- Evans RS, Takahashi K, Duane RT, Payne R and Lie CK. (1951) Primary thrombocytopenic purpura and acquired hemolytic anemia. Arch Intern Med. 87: 48-65. [PubMed.]
- Hauswirth AW, Skrabs C, Schützinger C, Gaiger A, Lechner K. (2007) Autoimmune hemolytic anemias, Evans' syndromes, and pure red cell aplasia in non-Hodgkin lymphomas. Jäger U. Leuk Lymphoma. 48: 1139-1149. [PubMed.]
- Puthenparambil J, Lechner K, Kornek G. (2010) Wien Klin Wochenschr. Autoimmune hemolytic anemia as a paraneoplastic phenomenon in solid tumors: a critical analysis of 52 cases reported in the literature. 122: 229-236. [PubMed.]
- Pelosof LC, Gerber DE. (2010) Paraneoplastic syndromes: an approach to diagnosis and treatment. Mayo Clin Proc. 85: 838-854. [PubMed.]