>Corresponding Author : Andrew S Ryser
>Article Type : Case Report
>Volume : 4 | Issue : 1
>Received Date : 12 Feb, 2024
>Accepted Date : 23 Feb, 2024
>Published Date : 27 Feb, 2024
>DOI : https://doi.org/10.54289/JDOE2400104
>Citation : Ryser AS, Handel S, Sabol JV, Meister D and McLaughlin J. (2024) Staged Extractions and Implant Placement for Maxillary Central Incisors: A Case Report. J Dent Oral Epidemiol 4(1): doi https://doi.org/10.54289/JDOE2400104
>Copyright : © 2024 Ryser AS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access
1Resident, CPT, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
2Assistant Program Director, LTC, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
3Program Director, COL, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
4Periodontist, Private Practice, Brentwood, TN, USA
5Prosthodontist, Private Practice, Brentwood, TN, USA
*Corresponding author: Andrew S Ryser, Resident, CPT, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
Abstract
A patient sought treatment at a prosthodontics practice to replace mobile maxillary centrals and exposed defective veneer margins on the maxillary laterals. Staged extractions and immediate implant placement were offered as the treatment option to preserve the hard and soft tissue around the implants and maximize the esthetic outcome. Staged extraction of adjacent teeth and immediate implant placement was performed to the maxillary central incisors. After osseointegration, custom impression copings were made to capture the gingival contours. The implants were restored with implant retained ceramic crowns and the maxillary laterals were restored with ceramic veneers. Although treatment time is lengthened staged extraction of adjacent anterior teeth and immediate implant placement can provide a predictable and successful treatment option to manage soft tissues and achieve a highly esthetic outcome.
Keywords: Implants; Esthetics; Immediate Implants; Immediate Provisionals; Staged Extractions; Prosthetic Dentistry
Introduction
A patient presented to a prosthodontics practice with mobile maxillary central incisors. Staged extraction of the central incisors and immediate implant placement and provisionalization of the implants was completed approximately 8 months apart. After osseointegration, custom impression copings were used to make a final impression of the maxillary central implants. Ultimately, the central incisors were restored with custom titanium abutments and ceramic crowns.
According to a systematic review by Ortega- Martinez et al. in 2012 immediate implant placement after extraction of teeth with a poor prognosis provides several advantages to include: reduced surgical procedures, shorter treatment times, proper implant positioning, preservation of alveolar bone, and soft tissue management [1]. A 2023 systematic review by Soegiantho et al. showed a survival rate of 83.7-100% for single immediately placed implants, stating that case selection was extremely important in the success of immediately placed implants [2].
In 2020, Khoury and colleagues described a papilla preservation concept for adjacent implants by implementing the "one-by-one" protocol. With the one-by-one protocol the authors were able to obtain satisfactory esthetic results with maxillary central incisor implants even though the extracted teeth were compromised periodontally. The protocol aims to preserve papillae and soft tissue architecture, which is usually compromised after extraction of adjacent teeth [3]. This case report demonstrates an excellent esthetic result with staged extraction and immediate implant placement.
Materials And Methods
A 38-year-old female patient in generally good health was referred to a prosthodontic clinic for extraction and implant restorations of maxillary central incisors (Fig. 1). The maxillary central incisors had Miller class 3 mobility, resorption of the roots, and exposed defective veneer margins (Fig. 2). The maxillary lateral incisors had recession of the gingiva exposing the defective margins of the veneers. The patient was concerned about the mobility of the central incisors, the recession causing the exposed margins of the veneers, and the diastema between the centrals. The patient desired fixed restorations to replace the centrals and was esthetically highly demanding.

Figure 1: Patient initial presentation.

Figure 2: Initial periapical radiograph.
The initial phase of treatment included oral hygiene counseling, a prophy, and discussion of treatment options. The patient was informed of the possibility of bone loss and papilla loss with extraction of both central incisors and immediate implant placement at the same time. The patient was offered a treatment plan of staged extractions and implant placement with provisionalization in order to preserve the soft tissue and bone. The patient accepted the plan for staged extractions and implant placement even though the treatment time frame would be extended.
The right maxillary central incisor was extracted, and an immediate implant was placed. The implant was torqued to 35 Ncm and was provisionalized using the patient's extracted tooth as the provisional crown on a temporary abutment (Figs. 3 and 4). Approximately eight months later the left maxillary central incisor was extracted, an immediate implant was placed, and the implant was provisionalized using the extracted incisor on a temporary abutment. The maxillary lateral incisors had previous restorations removed and reprepared for veneers. Custom impression copings for the maxillary central implants were fabricated using the provisional crowns to replicate the gingival contours (Figs. 5 and 6). The custom impression copings and a custom tray were used to impress the implants and veneer preparations of the maxillary lateral incisors (Figs. 7 and 8). The maxillary laterals were restored with lithium disilicate veneers, and the maxillary central implants were restored with custom zirconia abutments and lithium disilicate crowns (Figs. 9 and 10). This manuscript was written following the CARE guidelines on case reports.

Figure 3: Extraction of maxillary central incisor.
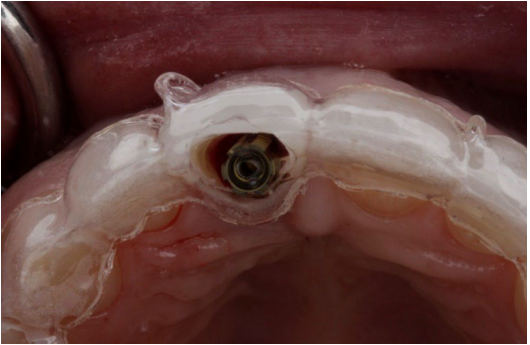
Figure 4: Provisionalization of immediate central incisor implant.

Figure 5: Facial view of tissue contours with implants placed.
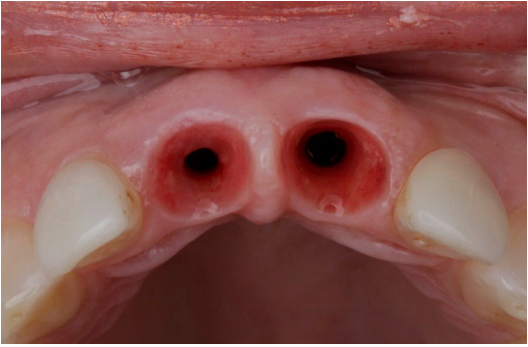
Figure 6: Incisal view of gingival architecture.

Figure 7: Custom impression copings being fabricated.
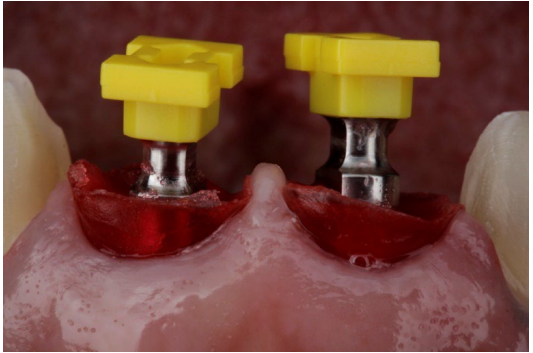
Figure 8: Custom impression copings placed intraorally.

Figure 9: Final restorations.
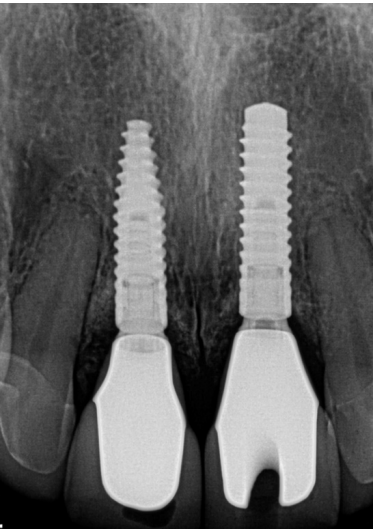
Figure 10: Final radiograph.
Discussion
Extraction of teeth can lead to changes in the hard and soft tissues at that extraction site [4]. According to Schropp et al. in 2003 there is a 50% reduction in width of the alveolar ridge in the first 12 months with two-thirds of that reduction occurring in the first 3 months [5]. According to a review by Hammerle and Tarnow in 2018, without additional treatment, changes to the alveolar complex following extraction is the main reason for soft tissue deficiencies prior to implant placement. Hammerle and Tarnow also stated that a common soft tissue deficiency between adjacent implants is a reduced papilla [6]. A reduced papilla can cause significant esthetic concerns that can be difficult to correct, and the papilla height is determined by the alveolar crest between implants. Extraction of adjacent teeth and replacement with immediate implants can compromise the papilla height and shape due to the unpredictability of tissue remodeling.
Staged extractions of adjacent teeth with immediate implant placement can help preserve the gingival contours, papilla, and bone. Immediate implant placement was defined by Schwartz et al. in 2000 as the placement of an implant into a site immediately after extraction of the tooth and considered to be a reliable and predictable treatment option [7]. The purpose of immediate implant placement and provisionalization is to maintain the gingival contours and papillae present at the time of extraction. Immediate implant placement for anterior teeth have reported success rates range from 93.5% to 100% [8]. The criteria for placement of immediate implants as described by Kumar in 2012 include: achieving osseointegration, consideration of site anatomy, soft tissue conservation and maximizing esthetics for the patient, restoring function, medical and dental status of the patient, the surgical technique utilized, and the preference/ experience of the clinician [9].
In 1998, Wohrle et al. first described provisionalizing immediate implants in the anterior region and in the years since the protocol has been found to be highly successful and provides stable gingival contours [10]. According to Meng et al. provisionalizing an immediate implant is a predictable treatment option that produces greater patient satisfaction. Meng and co-authors emphasized that immediate provisional-ization of implants is a clinical decision if primary stability is achieved, the provisional crown is free of contacts during articulation, and the patient is willing to follow post operative instructions [11]. Utilizing the patient’s extracted tooth as a provisional crown can be a highly effective way to provisionalized the implant if the clinical crown is of an acceptable shape, esthetically pleasing, and free of caries. According to Bhargava et al., using the patient's natural tooth for a provisional crown can help ease the anxiety of losing an anterior tooth, and provide a restoration that is the right size, shape, and color if the clinical crown is in good condition [12].
Conclusion
This case report demonstrates the staged extraction of teeth being replaced with immediate implants that resulted in a very positive outcome. Staged extractions of teeth with immediate implant placement can preserve papilla that otherwise might decrease in size or disappear if adjacent teeth were extracted at the same time and immediate implants were placed. Immediate provisionalization of the implants allows the patient to leave the day of surgery with anesthetic temporary prosthesis and gives the clinician controls of the gingival contours that can be replicated using custom impression copings when the implant is ready for the final restoration.
Although this case report required a prolonged treatment time, the outcome was exceptional, and the procedure demonstrates a predictable way to manage soft tissues when extracting and placing adjacent immediate implants. Further research is needed to determine the minimum time frame to wait between extractions of adjacent teeth and placement of immediate implants.
Disclaimer: The views expressed in this manuscript are those of the authors and do not necessarily reflect the official policy of the United States Government, the Department of Defense, the Defense Health Agency, the Department of the Army, the United States Army Medical Department, or Uniformed Services University.
References
- Ortega-Martínez J, Pérez-Pascual T, Mareque-Bueno S, Hernández-Alfaro F, Ferrés-Padró E. (2012) Immediate implants following tooth extraction. A systematic review. Med Oral Patol Oral Cir Bucal. 17: 251-261. [PubMed.]
- Soegiantho P, Suryawinata PG, Tran W, et al. (2023) Survival of Single Immediate Implants and Reasons for Loss: A Systematic Review. Prosthesis. 5: 378-424. [Ref.]
- Khoury G, Chamieh F, Fromentin O. (2020) One-by-one immediate dental implants: A papillae preservation concept for adjacent implants in a compromised periodontal case. Clin Case Rep. 8: 2664-2672. [Ref.]
- Chen ST, Wilson TG, Hammerle CH. (2004) Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and out-comes. Int J Oral Maxillofac Implants. 19: 12-25. [PubMed.]
- Schropp L, Wenzel A, Kostopoulos L, Karring T. (2003) Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 23: 313-323. [PubMed.]
- Hämmerle CHF, Tarnow D. (2018) The etiology of hard- and soft-tissue deficiencies at dental implants: A narrative review. J.Periodontol. 89: 291-303. [PubMed.]
- Schwartz-Arad D, Grossman Y, Chaushu G. (2000) The Clinical Effectiveness of Implants Placed Immediately into Fresh Extraction Sites of Molar Teeth. J. Periodontol. 71: 839-844. [PubMed.]
- JY Kan, K Rungcharassaeng, JL Lozada, G Zimmerman. (2010) Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: a 2to 8-year follow-up. Int. J. Oral Maxillofac. Implants. 26: 179-187. [PubMed.]
- Kumar G. (2012) Criteria for immediate placement of oral implants - a mini review. Biol. Med. 4: 188-192. [Ref.]
- Wohrle PS. (1998) Single-tooth replacement in the aesthetic zone with immediate provisionalization: fourteen consecutive case reports. Pract Periodontics Aesthet Dent. 10: 1107-1114. [PubMed.]
- Meng H-W, Chien EY, Chien H-H. (2021) Immediate implant placement and provisionalization in the esthetic zone: A 6.5-year follow-up and literature review. Case Rep Dent. 2021: 1-11. [PubMed.]
- Bhargava S, Namdev R, Dutta S, Tiwari R. (2011) Immediate fixed temporization with a natural tooth crown pontic following failure of replantation. Contemp Clin Dent. 2: 226-229. [PubMed.]