>Corresponding Author : Andrew S Ryser
>Article Type : Research Article
>Volume : 4 | Issue : 2
>Received Date : 18 March, 2024
>Accepted Date : 02 May, 2024
>Published Date : 06 May, 2024
>DOI : https://doi.org/10.54289/JDOE2400111
>Citation : Ryser AS, Akey MJ, Koutsopatriy IS, Sabol JV, Handel SE, et al. (2024) Split/Dual Tray Impression Technique with a Digital Workflow. J Dent Oral Epidemiol 4(3): doi https://doi.org/10.54289/JDOE2400111
>Copyright : © 2024 Ryser AS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Research Article | Open Access
1Resident, CPT, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
2Program Director, COL, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
3Assistant Program Director, LTC, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA
*Corresponding author: Andrew S Ryser, Resident, CPT, Department of Prosthodontics, Army Postgraduate Dental School, Postgraduate Dental College, Uniformed Services University, Fort Eisenhower, GA, USA
Abstract
Making an accurate impression is a crucial step in fabricating a removable prosthesis that fits the patient with retention, stability, and support. Numerous impressions materials and techniques exist for making dental impressions. The clinical technique discussed in this article utilizes a 3D printed custom tray, and a dual tray impression technique, to fabricate an immediate denture for a patient with terminal maxillary anterior dentition. This technique utilizes digital dentistry to make a well adapted impression that captures the anatomy of the soft tissue, functional margins, and compromised dentition using polyvinylsiloxane for the edentulous area and alginate for the dentate area.
Keywords: Digital Dentistry; Removable Prosthodontics; Impressions; Dentures; 3D Printing
Abbreviations: CAD-CAM: Computer Aided Design- Computer Aided Manufacturing
Introduction
The prevalence of edentulism is decreasing throughout the United States however the number of edentulous people is increasing due to the growth of the population and an increase in life expectancy [1]. The main causes of edentulism are dental caries and periodontal disease [2]. Extraction of teeth and immediate restoration with complete dentures has been done since the mid-1800s [3]. Transition to edentulism can be physiologically and psychologically traumatizing, especially when the patient does not receive an immediate prosthesis to replace the extracted teeth. Lavere in 1973 stated that “instant dentures are a necessity to prevent distress, anxiety, and embarrassment” [4].
An immediate denture is defined by the Glossary of Prosthodontic terms as a prosthesis fabricated for placement immediately following the removal of a natural tooth/teeth [5]. Immediate dentures provide many advantages to the patient to include:
1. The patient does not have to be without teeth while the mouth is healing from extraction of the dentition.
2. Reduced pain and inflammation due to the immediate denture acting as a protective splint while healing.
3. The prostheses allows the clinician and patient to test esthetics of tooth shape and shade.
4. Maintenance of speech and appearance which improves cooperation and psyche of the patient.
5. The patient usually adapts easier than waiting for healing to occur before delivering dentures [4,6].
Immediate dentures have several disadvantages compared to conventional dentures made from an already healed edentulous ridge including:
1. Immediate dentures will require relines as healing and resorption of the alveolar ridge occurs.
2. Patients with a compromised medical history may have increased chances of infection and healing may be delayed or compromised.
3. Additional treatment time for post deliver adjustments.
4. Immediate dentures cannot be assessed during the fabrication phase due to the inability to try them in mouth with teeth still present [4,6].
When fabricating immediate dentures two techniques have been described to make a final impression. The first technique is simply making a single impression to capture the remaining teeth and soft tissues simultaneously. A second option for the provider is to utilize a dual or split impression technique in which an impression of the edentulous area(s) is completed and then a secondary (split/dual) impression is made over that impression to capture the dentate area [7]. This technique report describes a novel technique using digital dentistry and 3D printing to fabricate a split/ dual tray to make an impression for a maxillary immediate denture.
Materials And Methods
A 65-year-old male presented to a prosthodontics practice with partial edentulism and remaining maxillary teeth that were non-restorable due to caries and periodontitis (Fig.1). The patient’s chief complaint was that he “was ready for a denture.” The patient’s maxillary posterior teeth were extracted approximately 8 weeks before the initial evaluation by a prior dentist who was preparing the patient for an immediate denture. A treatment plan of extraction of the maxillary dentition and restoration with an immediate maxillary complete denture was established, and treatment was initiated. Verbal and written consent was obtained from the patient. A diagnostic impression of the maxillary arch was made with alginate. The impression was poured, trimmed, and scanned using Primescan (Dentsply Sirona, USA). A custom tray was selected as the restoration and computer aided design- computer aided manufacturing (CAD-CAM) software (InLab, Dentsply Sirona, USA) was used to make a dual/ split tray using the following steps:
1. Design the edentulous area tray to encompass the edentulous area using 2 mm of spacer for polyvinylsiloxane material. Add positive and negative orientation notches to the cameo surface of the tray and a handle (Fig. 2). Selective pressure technique as described by Duncan was utilized for this case [8].
2. Print the edentulous tray, wash, cure, and remove supports (Formlabs, USA) (Fig. 3).
3. Place the edentulous tray on cast and place 4 mm of wax over the dentition to act as a spacer for the alginate. Scan the cast with the custom tray and wax utilizing a CAD-CAM software. (Primescan, InLab CAD, Dentsply Sirona, USA).
4. Design the dentate area tray and leave 0 mm of space so it contacts the edentulous tray intimately, add a handle to the second tray.
5. Print the dentate tray, wash, cure, and remove supports. (Formlabs, USA) (Fig. 4). Ensure the two trays fit together intimately, with orientation notches lining up (Fig. 5).
6. At the impression appointment try in trays and adjust as needed to ensure fit. Border mold using green stick plastic modeling impression compound and the edentulous custom tray (Fig. 6).
7. After border molding is complete, apply polyvinylsiloxane adhesive. Make a polyvinylsiloxane impression of edentulous area (Fig. 7). Inspect impression for any voids and inaccuracies, if satisfactory then apply alginate adhesive to cameo surface of first edentulous tray and place back in mouth.
8. Apply alginate adhesive to the dentate tray and place in mouth to take alginate impression of remaining dentition. Once alginate has set remove both trays together from mouth (Fig. 8).
9. Box and pour impression, trim final cast for fabrication of the immediate denture (Fig. 9).

Figure 1: Maxillary dentition.
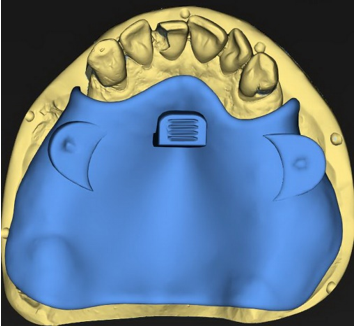
Figure 2: First tray being designed in InLab: cameo surface view.
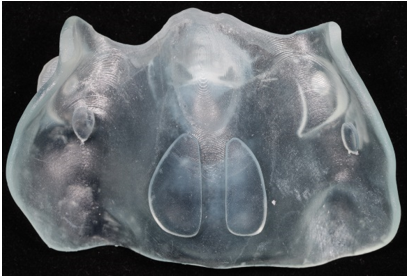
Figure 3: 1st tray printed: intaglio view showing selective pressure technique.

Figure 4: 2nd tray printed: intaglio surface view.

Figure 5: Dentate and edentulous trays together demonstrating an intimate fit.

Figure 6: Border molding complete with first tray.
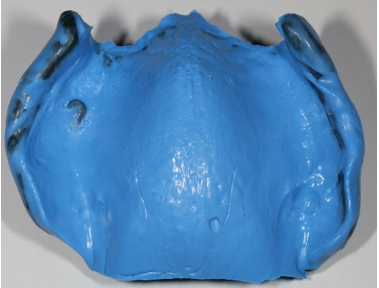
Figure 7: Polyvinylsiloxane impression complete with first tray.
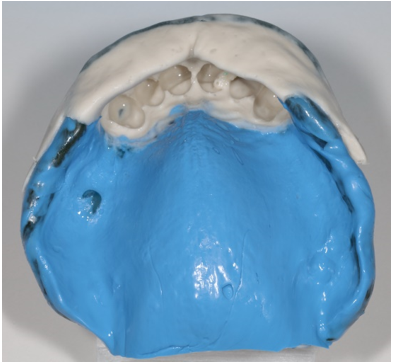
Figure 8: Dual alginate/ polyvinylsiloxane impression.

Figure 9: Final impression poured and trimmed.
Discussion
Accurate impressions are critical in fabricating an immediate denture that fits the mucosal surfaces of the denture bearing areas and replicates the anatomy produced by masticatory and facial muscles to achieve adequate support, retention, and stability [5]. According to Rudd and Morrow accurate casts made from accurate impressions should meet the following criteria:
1. All tissue surfaces that will be contacted by the prosthesis should be accurate and free of voids or bubbles.
2. The cast should include all of the maxillae and/or mandible available for support.
3. The peripheral roll should be complete and 3-4 mm deep [9].
The split impression technique was first described by Javid and colleagues from the Ohio State University in 1974 and since others have described different versions of the technique to achieve an accurate impression when posterior or anterior teeth remain and a denture needs to be fabricated [10]. The split impression technique allows the provider to use a custom tray to border mold and make an final impression of the edentulous area, and then a second custom tray or stock tray is used to make an impression of the dentate area with the first impression still remaining over the edentulous areas. Javid et al. described the split impression technique by making two custom trays and then taking the impressions and removing the anterior portion from the mouth first and then luting the two impressions together before pouring the impression [10]. Bolouri in 1977 went on to describe custom trays made with a key and keyway to securely fit the two trays together for proper orientation and removal of both trays as one piece from the mouth [11]. In 1982 Newton and Korbich described their split tray technique which included a window in the first tray for the second tray to sit into so both trays could be removed as one piece also [12].
The split/dual tray technique for immediate dentures provides the dentist with an opportunity to capture the edentulous area more accurately and incorporate functional borders with border molding [9]. The dentate tray allows the dentist to use a different impression material that will not compromise the positional stability of the teeth, damage fragile teeth, or prevent the tray from being removed due to tissue undercuts. The novel technique described in this article presents a digital pathway for creating a split/dual tray for immediate dentures. By using CAD- CAM the custom trays can be designed for the different types of impression materials that will be utilized for the impression and then be 3D printed. The digital pathway also allows the clinician or laboratory technician to design the trays to connect intimately which ensures the dentate tray sits on the edentulous tray properly. With an intimate fit the two trays can simultaneously be removed from the mouth as one unit and poured in stone without the need for luting the trays together or trying to figure out how to correct the orientation when positioning the individual pieces back together. The result obtained from the digitally designed custom split trays was a cast that accurately represented the patient’s anatomy and functional borders without damaging the periodontally and decayed remaining dentition.
Summary
This article provides a technique that aims to provide a digital pathway for the split/ dual impression technique. CAD-CAM programs afford clinicians the opportunity to quickly design custom trays with different features. While 3D printing allows for efficient fabrication of custom trays at a relatively low cost. The split/dual tray allows clinicians to capture the edentulous area of the maxillae or mandible more accurately. Obtaining an accurate impression allows the laboratory to fabricate a well-adapted prosthesis that extends to the functional margins on the soft tissues. A well-adapted prosthesis allows delivery to occur with less adjustments and allows the patient to receive a prosthesis that has great retention and stability.
Disclaimer: The views expressed in this manuscript are those of the authors and do not necessarily reflect the official policy of the United States Government, the Department of Defense, the Defense Health Agency, the Department of the Army, the United States Army Medical Department, or Uniformed Services University.
Acknowledgements: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no conflicts of interest.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no conflicts of interest.
References
- Slade GD, Akinkugbe AA, Sanders AE. (2014) Projections of US edentulism prevalence following 5 decades of decline. J Dent Res. 93(10): 959-965. [Ref.]
- Al-Rafee MA. (2020) The epidemiology of edentulism and the associated factors: A literature Review. J Family Med Prim Care. 9(4): 1841-1843. [Ref.]
- Richardson JA. (1860) Practical Treatise on Mechanical Dentistry. Philadelphia, Lindsay and Blakiston, 1610-1920 [Ref.]
- LaVere AM, Krol AJ. (1973) Immediate denture service. J Prosthet Dent. 29(1): 10-15. [PubMed.]
- (2017) The Glossary of Prosthodontic Terms. J Prosthet Dent. 117(5S): C1-e105. [PubMed.]
- Heartwell CM, Salisbury FW. (1965) Immediate complete dentures: An evaluation. The J Prosthet Dent. 15: 615-624. [PubMed.]
- Nayak D, Singhal R, Agarwal S, Hussain S, Javed B, et al. (2020) Immediate Denture: A Review. Int. J Scientific Research. 1-4. [Ref.]
- Duncan JP, Raghavendra S, Taylor TD. (2004) A selective-pressure impression technique for the edentulous maxilla. J Prosthet Dent. 92(3): 299-301. [PubMed.]
- Morrow RM, Rudd KD, Rhoads JE. (1986) Dental laboratory procedures. Complete dentures. St. Louis: Mosby. 1. [Ref.]
- Javid N, Tanaka H, Porter M. (1974) Split-tray impression technique for immediate upper dentures. J Prosthet Dent. 32(3): 348-351. [PubMed.]
- Bolouri A, McKinney TW. (1989) Two-stage impression making for complete dentures over loose, mobile supporting tissues. Compendium. 10(4): 196, 199-201. [PubMed.]
- Newton JB, Korbich M. (1982) An improved split-tray impression technique for immediate complete dentures. Gen Dent. 30: 332-333. [PubMed.]