>Corresponding Author : Pankaj Kumar
>Article Type : Case Report
>Volume : 4 | Issue : 3
>Received Date : 28 Jan, 2024
>Accepted Date : 09 Feb, 2024
>Published Date : 14 Feb, 2024
>DOI : https://doi.org/10.54289/JCRMH2400114
>Citation : Kumar P, Mukherjee S, Sethi A and Gupta S. (2024) Invasive Candidiasis Causing Diabetic Ketoacidosis. J Case Rep Med Hist 4(3): doi https://doi.org/10.54289/JCRMH2400114
>Copyright : © 2024 Kumar P, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Case Report | Open Access
1Junior Resident, Government Medical College, Chandigarh
2Junior Resident, Government Medical College, Kolkata
3Intern, Government Medical College, Chandigarh
4Associate Professor, Government Medical College, Chandigarh
*Corresponding author: Pankaj Kumar, Junior Resident, Government Medical College, Chandigarh
Abstract
Diabetic ketoacidosis (DKA) is a common yet fatal complication of diabetes mellitus which is characterised by uncontrolled hyperglycaemia, metabolic acidosis, and increased body ketone concentration. This preventable hyperglycaemic emergency accounts for more than 50,000 hospital days per year [1]. Infections, non-compliance to medication are the main precipitating factors for DKA, although myocardial infarction, stroke, trauma, and substance abuse may result in DKA. Clinical features of the same include nausea, vomiting, dehydration, pain abdomen, Kussmaul breathing pattern or even altered mental sensorium. Different types of infections can precipitate DKA, commonly of which are pneumonia, urinary tract infection, Oro-mucosal and aural infections. Careful evaluation and identification of precipitating factor should be made earlier for prompt treatment The aim of this case report is to review knowledge gaps in precipitating factors of DKA.
Keywords: Diabetic Ketoacidosis; Diabetes Mellitus; Invasive Candidasis; Fungal Infections
Abbreviations: DKA: Diabetic Ketoacidosis
Blinder Main Text
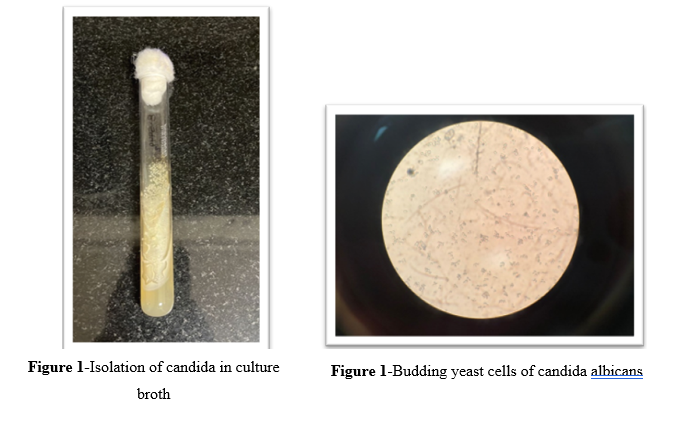
A 46-year-old woman known case of type-2 diabetes mellitus presented to the emergency with altered mental status and GCS was requiring intubation. On laboratory testing her results were; blood sugar levels- 541mg/dL, ketones- 6.7 mmoL/L and was diagnosed to have Diabetic ketoacidosis. While catheterization, fulminant white curdy discharge was noted at the vaginal introitus and a reddish rash was noticed over her vulva and inner aspect of the thighs. She was started on Broad Spectrum antibiotics and fluids with insulin and managed accordingly. After a few days in ICU her signs of recovery became evident as her GCS and ABG values started improving until she was finally extubated. Nevertheless, the precipitant of DKA in this patient remained an enigma until not one but two Routine Urinalysis showed Candida sp. smearing the full field under microscope which prevailed even after the catheter was changed. This wriggled our clinical suspicion and Blood cultures were ordered. The fungal cultures grew Candida (figure 1,2) and PCR revealed it to be Candida tropicalis manifesting as Invasive Fungemia which precipitated DKA in this patient. Subsequently a 2D-ECHO and Fundus examination were done which were negative for any evidence of endocarditis in the form of vegetations, new onset murmurs and Roth spots respectively.
The patient was started on oral Fluconazole mg once daily for 14 days on day 5 of hospital stay. The rate of recovery of fastened drastically within the next 48 hours. The patient was discharged and thereafter is on regular follow up on outpatient basis.
Discussion
Diabetes is an immunodeficient state that sets the stage for all sorts of bugs. Fungal pathogens are often found infesting the poor diabetic's body, with their prevalence not clearly defined in the literature so far. Among the fungal pathogens, Candida species primarily colonize the gastrointestinal and genitourinary tracts of humans as commensals. However, they can become a nuisance whenever changes occur in the environment of their ecological niche, manifesting as Oral (and Esophageal) Candidiasis, Cystitis, and other conditions. Most invasive fungal candida infections are caused by five pathogens: Candida albicans, Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei (Candida auris in some parts of the world) [2].
Diabetic ketoacidosis is a life-threatening metabolic complication that can be a presenting complaint of undiagnosed patient or wreak havoc in the life of patient with Type-1 DM. The presenting complaints often include acute abdomen, nausea, vomiting, and altered consciousness. Among the many known risk factors, such as intercurrent illnesses like acute coronary syndrome and insulin pump issues (e.g., dislodgement or blockage of infusion sets, lack of underlying infection(s) takes the spotlight [3]. of compliance with insulin therapy, the concurrent presence
In the literature that is available our case is the first of its kind where DKA was precipitated by Candidemia resulting from Candida colonizing the urinary tract of a 56-year-old lady who is a diagnosed case of Type-2 Diabetes for the past 15 years.
Conclusion
This case report highlights some important medical lessons – urinary tract infection caused by fungal infection should be kept in mind in patients of DKA. Candida species account for approximately 10% of all urinary isolates and is more common amongst nosocomial UTI [3]. Incidence of candidemia and candiduria causing DKA is still an enigma and should be looked for. In UTI precipitating DKA, we have to keep the suspicion of fungal infections as a cause of DKA in mind especially when it takes longer time to respond to antibiotics. Hence this case report highlights the importance of diagnosing the fungal UTI, obtaining blood and urine cultures to look for fungal infections and continue to treat these patients in the most effective manner.
Conflict of interest: None
Funding: Nil
References
- Abdul Rasoul MM, Mousa M, Al-Mahdi M, et al. Comparison of continuous subcutaneous insulin infusion vs. multiple daily insulin injection in children with type i diabetes in Kuwait: Glycemic control, insulin requirement, and BMI. Oman Med. 30(5): 336-343. [PubMed.]
- Turner SA, Butler G. (2014) The Candida pathogenic species complex. Cold Spring Harb Perspect Med. 4(9): a019778. [PubMed.]
- National Center for Health Statistics. National hospital discharge and ambulatory surgery data. [article online]. [PubMed.]